Point of Care Ultrasound POCUS Portable Handheld Machine for Emergency
Point-of-care ultrasound is not a smaller radiology. It is a different idea about when and where imaging happens. A clinician picks up a handheld scanner at the bedside. They ask one focused question. They read the answer in the same minute. POCUS is a question answered where the patient lies. It is no study filed for a report later. The clinician asks. The probe answers. The plan changes in the same breath, at the bedside, before the patient has been moved an inch.
The idea is old. The machine that delivered it is new.
For decades the scanner was a cart, tethered to a room. The change came once the electronics that form an image shrank into the probe itself. The story of that shrinking runs from the cart-to-handheld evolution through the steady miniaturization of the wand. The result fits in a coat pocket. It pairs with a phone the clinician already carries.
What made POCUS possible at the bedside
Point-of-care ultrasound answers a focused question where the patient is, in the minutes a decision allows.
Portability is the quiet revolution. A scanner that travels turns up at the trolley, the ward, the clinic an hour from a hospital. The clinical ideas waited decades for the hardware to catch up. The hardware caught up when the beamformer climbed inside the probe.
Emergency POCUS is built around a handful of focused exams. Each answers a narrow question fast. The sections below walk through them, one body region at a time. Each is a question asked where the patient is, answered fast enough to change the next decision.
Trauma and the search for hidden bleeding
The trauma application built the field’s reputation. A patient arrives after a crash. The abdomen is tender. The question that decides the next ten minutes is whether there is blood pooling inside where the eye cannot reach. A focused look at the spaces between the organs gives a fast answer at the bedside.
That look has a name and a sequence.
The FAST exam scans four windows in a set order. Extending it to the chest, the eFAST adds a look for blood or air around the lungs. The exam does not replace the detailed scan that follows in a stable patient. It sorts the patient who needs an operating room now from the one who can wait. In the crashing patient, minutes saved are the whole point.
The lung, read through its artifacts
A focused cardiac window answers whether the heart is filling and squeezing, in seconds.
Lung ultrasound surprised a field that once believed air made the lung invisible to sound. The trick is that the lung is read through the artifacts the pleura throws back. A clinician reads the signs, not the tissue.
A healthy lung shows two of them.
It shows horizontal repetitions, the normal A-line pattern. It shows a shimmering slide as the layers move. A lung filling with fluid throws vertical beams that multiply as the water rises. A collapsed lung erases the slide, the sign of a pneumothorax found at the bedside. From these few signs a clinician separates heart failure from pneumonia.
The signs can be counted and sequenced.
Counting the vertical beams can be done by eye or by an automated B-line counter. The whole sweep is taught as a named routine, the BLUE protocol for bedside lung scanning. The lung exam became a frequently reached-for part of emergency POCUS, since the findings are quick to learn and fast to read.
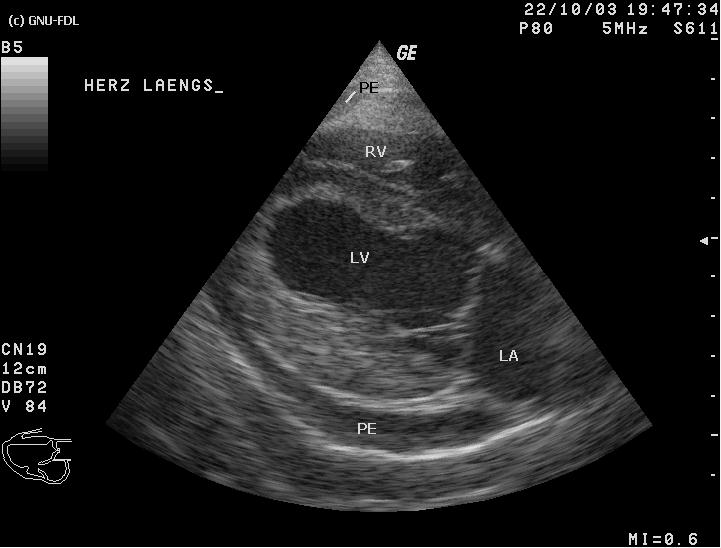
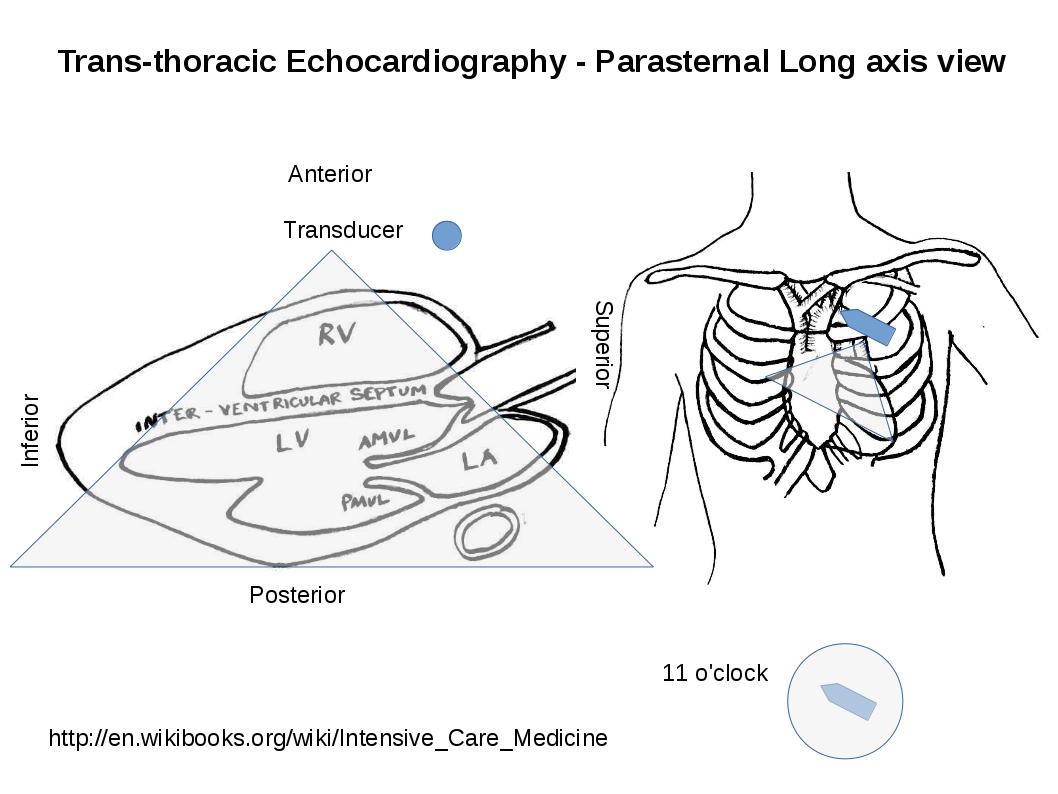
The heart, asked four blunt questions
A focused cardiac look does not attempt a formal echocardiogram. It asks four blunt questions a sick patient’s life can turn on. Is the heart squeezing. Is the right side strained. Is the big vein full or flat. Is there fluid in the sac around the heart, pressing it closed. None of these needs a cardiologist to answer at the level a resuscitation demands.
Each answer steers the next move.
A heart that barely squeezes wants different care from one choked by fluid in its sac. A swollen right side points at a clot on the lung. The focused look does not name every cause. It narrows the field fast enough to start the right treatment as slower tests run.
The shock survey, several questions at once
When a patient’s pressure falls and the cause is unclear, POCUS offers a rapid survey that asks several of these questions in sequence. The clinician looks at the heart, the veins, the lungs, the abdomen, the aorta in a few minutes. Is the heart too weak. Is the patient bleeding. Is fluid choking the heart. Has a clot blocked the lung. Has an aneurysm in the aorta burst.
The survey replaces a guess with a look.
It does not name the cause with certainty. It narrows the possibilities fast enough to start the right treatment as slower tests run. For a patient sliding toward arrest, that head start is often the difference. The clinician looks at each in turn and lets the images sort them.
Who uses POCUS, and the training behind it
POCUS began with emergency physicians. It spread fast. Critical-care doctors took it to the intensive unit. Anaesthetists took it to the block and the line. Surgeons, midwives, paramedics, rural family doctors: each found a focused exam that changed a decision. The tool is now a basic skill across many specialties, near the place the stethoscope holds.
The skill is learned by holding a probe.
A clinician does not learn ultrasound from a book alone. They learn it by scanning, under guidance, on real patients, until the views come without thought. A handheld put a scanner in every learner’s hand at a cost a teaching program could bear. The guidance software many devices carry coaches a beginner toward a standard view. It flags a finding for a second look. A novice builds a safe, useful skill in weeks that once took months. Training is the line between a focused exam that helps and one that misleads. A clinic that invests in it gets exams it can trust. One that hands out devices without teaching gets blurry pictures and shaken confidence. The machine shrank. The need to learn it well did not.
The limits a focused exam carries
A focused exam is powerful for the question it was built to answer. It is weak the moment it strays past that question. A FAST scan that misses a small bleed does not rule the bleed out. A clear lung does not promise a healthy heart. The exam answers what it was aimed at, no more.
A negative scan is not an all-clear.
The discipline of POCUS includes knowing what a normal picture does not say. A clinician reads the focused exam as one input among several, weighed beside the history, the examination, the vital signs. A finding changes the plan. The absence of a finding rarely closes the case on its own. The exam that saves a life in the right hands can mislead in hands that ask it for more than it can give. Respecting the edge of the question is as much a skill as acquiring the image. The strongest POCUS clinicians are the ones quickest to say what their scan did not show. They treat a clean image as a reason to keep thinking, never a reason to stop.
A bedside scan rules a finding in with confidence. It rules one out only within the narrow window the probe could see. The lung that slides freely in one spot may have collapsed in another the probe never reached. The abdomen clear of free fluid today may bleed an hour from now. A clinician who carries that humility scans often, acts on what the image shows, and keeps watching the patient for what it could not.
Governance, records, and the image that is kept
A focused exam is still a medical act. The image it produces belongs in the patient’s record, the same as any other. A study captured at the bedside has to be saved, labelled, then stored where the rest of the record lives. A device that exports cleanly into the clinic’s systems makes that easy. One that traps images in an app makes it a chore, and a chore skipped becomes a gap in the record.
The saved image protects the patient and the clinician alike.
It documents what was seen, and when, and on what grounds a decision was made. It lets a colleague review the finding later. It feeds the quality review that keeps a service honest about its hits and its misses. Governance asks one more thing of a POCUS programme: a clear account of who is trained to scan, on what, to what standard. A device handed to an untrained user, with no record kept and no review behind it, is a risk dressed as a convenience. A programme built on training, on documentation, on review turns the same device into care a clinic can stand behind. The picture lasts a second on the screen. The record of it lasts as long as the patient’s chart, and it carries the weight of the decision made on it.
How POCUS differs from a full study, and why it matters
The line between point-of-care and comprehensive ultrasound runs deeper than size, and it repays drawing in full, since the difference shapes how the two are used and why a clinic needs both. A comprehensive study sweeps an organ system from end to end. It documents every structure on a checklist. It produces a report a specialist signs, on a console with the power and the screen for the task. A point-of-care exam asks something narrow and urgent. Is there blood in the abdomen. Is the heart filling. Is this lung sliding. The clinician who asks the question is the clinician who acts on the answer. The loop from suspicion to image to decision closes in moments instead of hours. The two are not rivals. They are different tools for different jobs. A focused exam at the bedside saves the minutes a crisis spends. A comprehensive study answers the thorough question a focused one cannot. A clinic that grasps the split keeps a handheld at the bedside for the urgent narrow question, and sends the exhaustive work to the console that was built for it. The handheld did not replace the cart. It added a fast, mobile tier beneath it, always present, always to hand. The patient gains from the pairing. The image that has to travel reaches the bedside in a pocket. The image that has to be exhaustive waits for the room that can produce it. Reading the two as a pair, rather than a contest, is the habit that uses each one well.
POCUS is a focused question, answered where the patient is.
Each exam above asks one such question, fast enough to change the next decision. Together they form the discipline that emergency and critical-care medicine now lean on, day and night, at the trolley and the bedside, wherever a sick patient cannot wait for the room.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.