One curved probe, run at a low pitch, reaches the whole deep belly: the liver and gallbladder, the kidneys and spleen, the bladder and the aorta against the spine. Reading those organs is the daily work of abdominal ultrasound, the same fan-shaped gray picture turned to one question after another. A fatty liver, a stone in the gallbladder, a kidney swollen above its blockage, an aorta stretched toward bursting: each is the same probe and the same picture, read by a hand that knows where to look and what the gray means.
The curved probe for the deep belly
The shape is the whole idea. A convex probe carries its crystals along a curved face. That curve fans the sound into a wide wedge from a footprint small enough to sit in the soft hollow below the ribs. The frequency runs low, near two to five megahertz. These long waves push deep into the body before they fade, reaching the back of a swollen liver or the aorta pinned in front of the spine. The deep picture they bring back is soft-grained, the texture coarser the further down it comes. The machine sharpens what it can. A focal marker dragged to the depth of the target tightens the beam exactly where the organ sits. Harmonic imaging, rebuilt from the echoes the tissue itself returns, lifts some of the haze a heavy belly throws over the view. For a large patient the frequency drops lower. The picture turns softer at that depth, the price of reaching so far down. The convex probe is a deep-reaching tool first. Every belly scan begins from that one choice of shape and pitch.
A few controls turn that reach into a readable picture. Depth is opened until the far organ sits a little inside the bottom edge of the screen, the field cropped close so the target is drawn as large as it can be. Gain lifts or lowers the brightness of the whole picture. Time-gain compensation, a column of sliders, trims that brightness band by band so the picture holds an even tone from top to bottom. The focal marker rides down to the depth in question. These few dials, set together, pull a clear picture out of a difficult belly.
Reading the gray picture
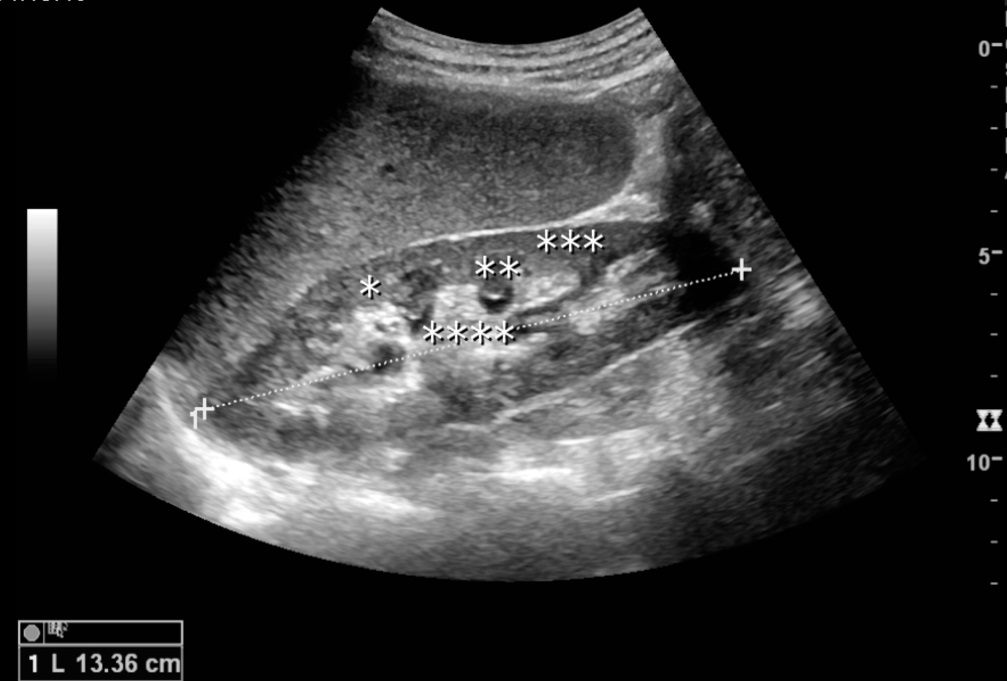
A kidney in long axis on the convex probe, the liver lying above it as the gray reference. The bright centre is the renal sinus, its fat and vessels; the darker rim is the cortex, a shade below the liver. The asterisks are the author’s labels for structures in the sinus, and the dotted line with its 13.36 cm reading is a length caliper, not part of a live scan. Image: Kristoffer Lindskov Hansen et al., CC BY 4.0.
A deep organ is named by its grain, the brightness it throws back held against the organs around it. The liver sets the reference, an even mid-gray the whole belly is judged by. Against it a kidney looks a shade darker in the cortex, its centre bright with sinus fat. The spleen comes close to the liver, smooth all through. The pancreas is the hard one, a soft gray gland that bowel gas keeps stealing from view. Learning these few tones is learning to read the belly at all. The step in brightness from the liver to the kidney beside it is read on its own, a jump that flags a bright, fatty liver.
Fluid is the great clarifier. Bile in the gallbladder, urine in the bladder, a pocket of ascites in a flank: each runs jet black and passes the beam on without loss, throwing a bright wall of echoes on the far side that marks it as liquid. A solid mass holds its own gray, with no such bright wall behind it. The diaphragm arcs as a bright line above the liver and the spleen. A clean copy of the liver thrown across that line is an echo trick, the kind of mirror the deep belly plays on a reader who forgets that sound can bounce.
Fluid leaves a second mark below it. A bladder or a cyst brightens the tissue directly behind it, a wash of extra echo called posterior enhancement, the beam passing through clear liquid and striking the far side with more strength than its neighbours. A small bright crystal can send back a fine tail of echo that shimmers down the screen, a clue to a speck the eye would miss. The near field, close under the probe, often fills with a low haze that no gain setting fully clears. A reader learns these signatures as part of the grammar, marks the beam itself leaves on the picture.
The picture moves. That movement carries its own reading. A vessel pulses with the heartbeat. Bowel squirms with the slow churn of the gut. The diaphragm slides up and down with each breath, sweeping the liver beneath it. A frozen frame loses all of this. A reader watches the live screen for a beat or two, since a structure is often known by the way it moves as much as by its gray.
Orientation is fixed by habit. The marker on the probe is turned so the patient’s head or right side falls to one set edge of the screen, the same on every study. Grain and position together name the organ, both read before a single measurement is taken.
Working the belly in order
A belly scan is a tour taken in a fixed order, the probe carried along the same route each time so no organ is missed. The patient lies flat, ideally fasted. An empty stomach holds the gallbladder full for reading. A quiet gut throws less gas across the windows. A held breath earns its place at the ribs: a deep breath drops the liver and the right kidney down below the costal margin into clear view. The same trick on the left brings the spleen within reach. The exact path, from the right upper quadrant down to the pelvis and organ by organ between, is set out step by step in the quadrant-by-quadrant scanning sequence.
The organs themselves are read in a settled order too, each found, sized, and checked before the probe moves on. The liver and the gallbladder, the pancreas and the spleen each have their landmark and their window, laid out in the organ-by-organ sweep of the upper abdomen. The discipline matters more than any one window. A belly read by wandering, the probe drifting wherever the hand fancies, skips the quiet organ and misses the finding a system would have caught. The same route run every time builds a habit that checks each space whether trouble is suspected there or not.
The belly is reached through a few set windows. Below the ribs on the right, a probe angled up under the costal margin looks through the liver at the gallbladder and the right kidney. Between the ribs, an intercostal slide catches a high liver or a spleen tucked under the diaphragm. A window between the lower left ribs, with the patient rolled toward the right, is the surest way onto a high spleen. In the flank, the kidney is found in its bed of fat. Low over the pubic bone, a full bladder opens the pelvis. The same handful of windows, learned once, serve every patient on the table.
The measurements a study records
A belly scan is not only a picture. It carries a handful of numbers, each read off a set plane and written into the report. The liver is measured head to foot in the line below the right collarbone, a span that reaches about fifteen or sixteen centimetres in a healthy adult. A span past that, with a rounded lower edge, reads as an enlarged liver. The spleen is sized along its length, held under about twelve centimetres. Both organs are read at their longest, the scan plane turned until the full length lies on the screen.
A kidney runs some ten to twelve centimetres from pole to pole. The two sides are compared for one that has shrunk or swollen. A difference of more than a centimetre or two is itself a finding to record.
The thin tubes carry numbers too. The common bile duct is followed to the porta and measured across its channel, a calibre that sits near six or seven millimetres. The portal vein and the bile duct run side by side at the porta, told apart by the flow inside them. The aorta is the one number a belly scan never skips: measured outer wall to outer wall in cross-section, a width of three centimetres or more takes the name of an aneurysm and is watched or sent on by its size. The two iliac branches are followed a little past the split, since an aneurysm can sit there too.
The bladder is gauged by volume, its three diameters multiplied to read the urine left after a patient has tried to empty. A wall is measured where it should run thin, a gallbladder wall past about three millimetres counted as thickened. Written down, a measurement outlives any memory of the screen. The next clinician reads the figure for what it is.
What a complete study covers
A full abdominal study is a defined list, not a free look. It sets down which organs must be seen, in which planes, and what must be measured on each, so two readers describe the same belly the same way. The same list applies whether the scan is a quick bedside look or a full department study. The professional standard for that list, the views and the documentation a complete scan is held to, is summarised in the AIUM practice parameter for an abdominal ultrasound. A handheld convex probe can meet much of that list at the bedside, organ by organ, as long as the operator works to the same plan a cart-based machine is held to. A smaller device follows the same plan.
The point of the standard is completeness. A study that skips an organ is half a study. A number read off the wrong plane misleads. Holding the bedside scan to the written list is what keeps a quick look honest, the record built the same way whether the picture comes from a console or a pocket device. The record is as much the work as the picture. Each organ seen is captured in at least one labelled image, named and marked with its side, so the study can be read back by someone who never held the probe. A measurement is written with the plane it came from. A normal organ is noted as seen and normal, so a later reader knows it was checked. This discipline of writing down is what turns a look on a screen into a study that stands in the notes.
Before the probe touches down
The picture is half-won before any gel meets skin. A patient fasted for a few hours brings a distended gallbladder and a calmer bowel, the upper belly far easier to read. The pelvis wants the bladder full. A bladder stretched with urine throws a clear window down onto the uterus or the prostate behind it, the deep pelvic organs read through that pool.
Position is the other free gain. Rolling the patient onto one side floats bowel gas off a target and slides a solid organ down into a cleaner window. Sitting the patient up drops the liver and drains free fluid to a low corner where the probe can find it. The body is moved to serve the beam. A minute spent settling the patient saves five spent fighting a bad angle.
The patient is part of the setup. A warm word and a clear breath cue win more than any dial: a patient who holds a breath on command brings a hidden organ into clear view. Warm gel spread on the skin carries the sound across the gap into the body. For an internal view the probe takes a cover and a clean barrier. Gloves and a clean probe between patients are part of the same minute, the habit that keeps a shared device safe.
The organs and the spaces
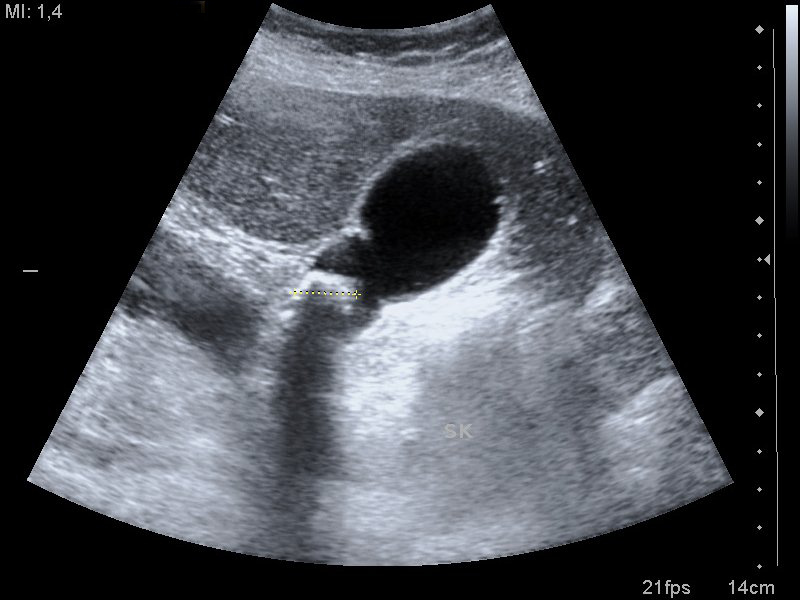
A gallstone in a bile-filled gallbladder. The gallbladder is the dark anechoic oval; the bright focus at its lower wall is the stone, dropping the clean dark shadow below it that marks something dense the beam cannot cross. The short yellow dotted line is the operator’s caliper, and the “SK”, “MI 1,4” and “14 cm” are the machine’s own labels. Image: Nevit Dilmen, CC BY-SA 3.0.
The curved probe’s round runs across the solid organs and the spaces between them, each its own reading on its own page. The liver fills the right upper quadrant, read for its texture and its edge. A coarse, shrunken liver with a knobbly surface is the picture of scarring, graded in the assessment of a cirrhotic liver. A lump that breaks the even grain is followed up as one of the masses that hide inside the liver. The gallbladder hangs beneath, watched for the stones that gather in it and the inflamed wall that sends a patient in doubled over. The spleen sits opposite, sized when it grows past its bound in the measurement of an enlarged spleen.
Some of the belly keeps no page of its own. The pancreas lies deep behind the stomach, a soft gland the gut gas guards closely, read through the window a full stomach of water can open. The adrenal rides above each kidney, a small gland seen only when a mass swells it. The bowel loops fill the spaces between the solid organs, followed for a wall grown thick or a loop blown up and still. The retroperitoneum runs behind it all, the great vessels and the drainage of the kidneys laid along the back wall. A tail of pancreas lost behind gas is the commonest blind spot in the upper belly.
The kidneys lie deep in the flanks, found through the liver on the right and the spleen on the left, scanned for the stone that blocks them and the swelling that backs up behind it. The bladder rounds out the pelvis, a dark, easy target measured for the urine left after voiding. The aorta runs the midline ahead of the spine, read for the widening that warns of an aneurysm. The flanks and the pelvis are swept for free fluid pooling where it should not be. The gut itself is followed for a swollen, motionless loop or a thick-walled, tender segment. Each of those spaces has a low corner where free fluid gathers first, the lowest point in the space.
Color and flow in the belly
Color Doppler adds the one thing the gray picture leaves out: motion. A wash of color over a dark tube fills it when blood is moving through, the surest way to know a vessel at the porta from a bile duct that carries none. The portal vein, the hepatic veins, the renal arteries, the aorta and the cava all declare themselves by their flow. A dark tube that fills with color is a vessel. The reader moves on. Flow tells more than identity. The push of color in the aorta marks a living pulse. A swirl of it inside an aneurysm shows the blood still moving past the clot laid down on the wall. Behind a hard stone, color can throw a quick flicker of false signal, the twinkle that helps catch a small stone the gray picture nearly missed. Spectral Doppler takes it further, tracing the waveform of a renal or portal vessel for a closer read. Color costs nothing to switch on, one more answer the same probe gives for free.
Gas, ribs, and fat
The belly fights back at every turn. The fight is mostly against air. Gas trapped in the bowel scatters the beam into a white, meaningless glare that hides whatever lies beneath it.
A rib drops a clean dark bar of shadow across the picture. A deep layer of fat drinks the signal before the echo can climb back. These are not faults in the machine. They are the body’s own walls, thrown up against a beam that lives on clear, fluid-filled paths.
The counters are old and physical. Press the probe down slowly to squeeze the gas aside, the graded compression that opens a window onto a tender belly. Roll the patient to float the gas up and slide a solid organ into the gap it leaves. Ride the breath to carry a target out from behind a rib. For the heaviest patient the answer is the dial, a lower frequency or the harmonic mode that claws a usable picture out of a body the beam can barely cross. Each is a move of the hand alone.
The shadows carry a message of their own. A stone or a rib throws a clean shadow with sharp edges, the sign of something dense the beam cannot pass. Gas throws a dirty shadow, a ragged gray band flecked with noise, the sign of air breaking the beam up. The clean band behind a gallbladder marks a stone. The ragged band drifting in the upper belly marks a loop of gassy bowel. One darkness carries two meanings. The edge of the shadow is what tells them apart.
A focused screen, not the whole study
The handheld belly scan is a fast answer to one pressing question. It sorts a sick patient into broad bins: a blocked kidney or a free one, a full bladder or an empty one, a flank with fluid or a dry one. Each of those answers turns a decision at the bedside without the wait for the department, the look that buys the hours a sick belly cannot spare.
The focused scan rewards repeating. A belly read once is a single frame of a moving story. The same look taken again an hour on can catch the fluid that has gathered, the loop that has swollen, the bladder that has filled, a change no single snapshot would show. The bedside probe is cheap to bring back. Two quick scans an hour apart often tell more than one careful study frozen in time. A clot seen to grow, a pool seen to spread: the second look catches it.
The skill is knowing the edge of the tool. A clinician who reads a clean bedside scan as a clean belly, then stops, has trusted a screen past its reach. The focused look lowers the odds of loud trouble. The fine disease it was never built to find belongs to the full study.
A screening eye, used as a screening eye, is a powerful thing. Trusted as the full study, the same look becomes a quiet danger.
The honest list of what it can miss is short and important to know. An early appendix, a small pancreatic growth, a flat sheet of bowel disease, a fine texture change too faint for a pocket screen: these belong to the full study and the trained eye. A clean handheld scan lowers the chance of serious trouble in front of the clinician. The subtle, early disease is the work of the full study and the department behind it. Knowing that edge is what lets the bedside scan be trusted for exactly what it does.
The convex probe at the bedside
Carried in a pocket, the curved probe brings the belly’s first deep answer to where the patient lies.
Common questions about abdominal convex-probe ultrasound
What does a convex probe show in the abdomen?
The solid organs and the great vessels. One ordered sweep takes in the liver and gallbladder, the pancreas, the spleen, the kidneys, the bladder, and the aorta down the midline. It also reads free fluid in the flanks and a swollen loop of bowel, and it carries a pregnancy scan through the abdominal wall.
Why does the belly need a convex probe?
Depth. The belly lies deep. The convex probe is the tool that reaches it, its low frequency near two to five megahertz sending sound far enough to find a liver edge or the aorta against the spine. A linear probe runs at a high frequency that draws fine detail in the first few centimetres. Its beam fades well before a deep organ. The convex wedge also lays a whole organ across the screen at once.
Do you need to fast before an abdominal ultrasound?
For the upper abdomen, usually yes. A few hours without food leaves the gallbladder full for reading and quiets the gas in the gut. A pelvic scan asks the opposite of the bladder, which is kept full to open a window onto the organs behind it.
Can a handheld convex probe replace a full abdominal scan?
For a focused bedside question, it answers well: a blocked kidney, free fluid, a full bladder, a widening aorta. The complete diagnostic study, with its full written list of views and measurements, runs on a department machine in the hands of a trained sonographer.
What is hardest to see on a belly scan?
Anything hidden behind gas or bone. The pancreas, tucked behind the stomach, is the classic hard one, often lost to bowel gas. A deep organ in a large patient fades into grain. A structure behind a rib needs a held breath to bring it into a window.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.