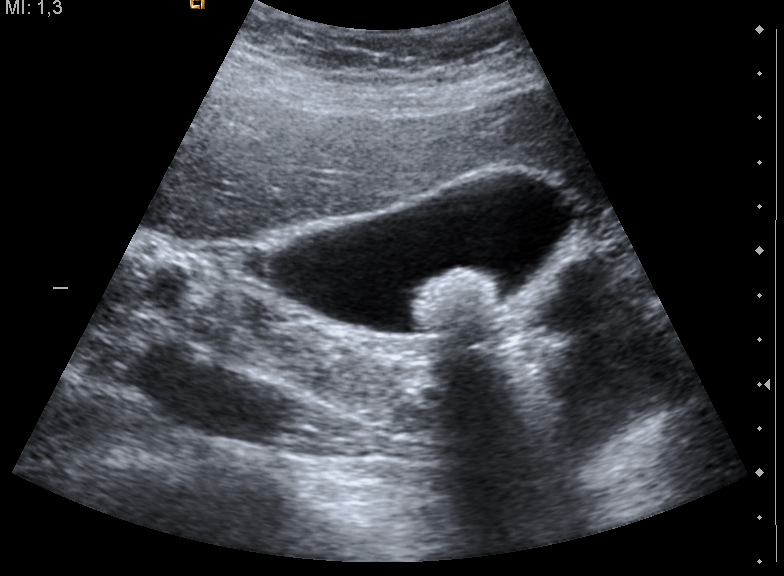
Gallstones are among the commonest findings the abdominal probe turns up; ultrasound is the test that finds them better than any other. A stone in the gallbladder has a signature clean enough that a handheld probe at the bedside can call it with confidence: a bright spot in the dark bile, a black shadow falling behind it, and a tumble downhill when the patient rolls. The scan here is not asking whether the gallbladder is inflamed, a question that belongs to the page on cholecystitis; it is asking a plainer one, whether stones are present at all and what they are, since the answer steers everything from a planned operation to the search for a cause of pain.
A gallstone on the handheld probe: a bright focus throwing a clean shadow behind it. Credit: Wikimedia Commons (CC).
A stone is bright, it shadows, and it rolls.
Bright, shadowing, and mobile: a stone shows all three; a polyp holds still and a fold throws no shadow.
Bringing the gallbladder cleanly into view, the roll onto the left side and the held breath, sits in the pages on the abdominal sequence; the inflamed, tender gallbladder is the work of the cholecystitis page. The stones themselves are the work here, their marks and their mimics.
The three marks of a stone
A gallstone announces itself by three signs together, and reading all three instead of settling for one is what separates a confident call from a guess. The first is the stone itself, a bright echogenic focus sitting in the black bile of the gallbladder, its surface throwing back a strong echo where the surrounding fluid throws back none. The second is the shadow, the clean dark band that falls straight behind the stone, where the dense stone blocks the beam and swallows the sound, leaving nothing to return from the strip of tissue beyond it; this acoustic shadow is the surest of the three, since many bright things sit in a gallbladder; only a stone-dense object casts a sharp, clean shadow behind it. The third is mobility, the stone rolling to the lowest point of the gallbladder when the patient turns from back to side, obeying gravity as a free stone must, where a polyp fixed to the wall stays put. The three signs lean on one another: a bright focus without a shadow may be sludge or a fold, a shadow without a clear focus may be a loop of gas in front, a mobile bright spot with a clean shadow that slides downhill when the patient rolls is a stone and little else. Size shapes the picture too, a large stone shadowing boldly and a cluster of small ones throwing a broken, speckled shadow; a stone packed against many others moves little for want of room. A clinician who hunts for the full triad, who rolls the patient to watch the bright focus slide and confirms the shadow falls sharp behind it, calls a stone with a certainty that no single sign on its own can give; such a reader sidesteps the traps that catch an eye content with a bright spot alone.
The shadow is the surest of the three.
Reading the shadow well
The shadow is the sign this scan leans on hardest, and learning to read it well repays the effort. A true stone shadow is clean and sharp-edged, a black band with crisp borders thrown straight back along the beam, darkest when the focal zone is set at the stone and the gain pulled down. Gas throws a different shadow, grey and ragged and flecked with noise, the dirty shadow of bowel that should never be taken for the clean one of a stone. The opposite trap is the bright focus that throws no shadow at all but a trail of fine repeating echoes behind it, the comet-tail or ring-down of cholesterol crystals lodged in a thickened gallbladder wall, a sign of adenomyomatosis that mimics a stone’s brightness without its shadow. Telling the clean shadow from the dirty one and from the comet-tail is the daily craft of reading a gallbladder, the line between a stone, a loop of gas, and a wall studded with crystals.
The shadow has to be coaxed from a small stone. A pebble below a few millimetres may swallow too little of the beam to cast a visible band until the focus is dragged down to its level and the beam narrowed onto it; a shadow that flickers into view as the focal marker passes the bright spot is the confirmation a faint stone needs. Set the machine to bring the shadow out, and a stone the eye nearly walked past declares itself at once.
The shadow tells the stone from the rest.
The gallbladder packed with stones
When the gallbladder is packed full enough of stones that no bile is left to see, the ordinary picture vanishes and a different sign takes its place. Instead of a black sac with bright stones inside, the probe finds a curved bright line, then a thin dark space, then a dense shadow swallowing everything behind: the wall, the echo of the topmost stones, and the shadow they cast, a pattern named the wall-echo-shadow sign. The gallbladder has collapsed around its stones and reads as little more than a bright arc with a black hole behind it. The three pieces stack in a fixed order, the near wall, then the bright cap of the topmost stones, then the shadow that buries the rest, a sandwich the eye learns to recognise at a glance.
The packed gallbladder is the one a beginner walks past. A bright curve with a shadow can be mistaken for a loop of gas-filled bowel; the gallbladder, hidden inside its own shadow, is declared absent or simply missed. The clue is the layered look, the wall and the stones and the shadow stacked in order where bowel gas gives a messier, shifting blur; a clinician who knows the wall-echo-shadow sign finds the stone-stuffed gallbladder where another sees only gas and moves on. The same trap swallows the contracted, fibrotic gallbladder of long-standing disease, shrunken to a bright sliver the inattentive eye writes off as bowel.
A gallbladder full of stones can look like gas.
Stones, sludge and polyps
Three things sit inside a gallbladder and the bedside scan must tell them apart, since each means something different. A stone is bright, shadows and rolls. Sludge is the soft middle case, a grey sediment that layers in the dependent bile and shifts slowly when the patient turns, casting no shadow, being too soft to block the beam, a sign of stasis whose deeper reading sits on the cholecystitis page. A polyp is the fixed one, a soft-tissue lump growing from the wall that neither shadows nor moves when the patient rolls, staying anchored where a stone would fall away. A stone may sit still in a contracted gallbladder for want of room; stillness alone never rules a stone out, the shadow settling what movement cannot.
Movement and shadow sort the three. Roll the patient and watch: the stone slides downhill and shadows, the sludge creeps and does not, the polyp stays welded to the wall. A bright thing that neither shadows nor moves is a polyp until proven otherwise; a polyp past a certain size earns its own follow-up for the small chance it hides something worse, a reading that belongs to the formal study over the bedside glance. The commonest error is to call a small polyp a stone or a non-shadowing stone a polyp; the roll and the shadow, taken together, keep the two from trading places. The roll is the cheapest test there is.
Stones fall, sludge creeps, polyps stay.
The small stone and the hidden one
Not every stone shows its full signature; the small ones are the hardest. A stone below a few millimetres may be too small to cast a clean shadow, showing only as a bright fleck that the eye cannot separate from a fold or a speckle of noise; tightening the beam to the spot and watching for the faintest shadow as the focus is dragged to its depth is the trick that brings out a shadow a careless setting would miss. Tiny stones and coarse sludge shade into one another, the microlithiasis that a bedside scan can suspect and only a careful study confirms.
Position hides stones as readily as size. A stone wedged up in the neck of the gallbladder sits where the bile is thin and the walls crowd in, easy to scan straight past unless the neck is followed deliberately to its tip; that impacted neck stone is the one that turns dangerous; the inflammation it triggers is read on the cholecystitis page. Stones that have left the gallbladder for the bile duct slip beyond the easy reach of a handheld probe, the duct hidden by gas and depth, the search for a stone in it a job for the fuller study.
A small stone hides in a fleck; a neck stone hides in plain sight.
The twinkle that lights a stone
Colour Doppler carries a trick that turns a doubtful stone certain. Aimed across the bright focus, it sometimes throws a chaotic flash of colour behind the stone, a mosaic of reds and blues with no flow to explain it, the twinkle artefact thrown back by the rough crystalline surface. A stone that twinkles is a stone confirmed, the artefact lighting up small stones and the ones tucked in awkward corners that grey-scale alone leaves in doubt. It earns its keep above all for the small stone in the neck or the duct, where a faint focus and a weak shadow leave the eye unsure until a burst of twinkle settles the question.
A stone that twinkles is a stone.
What a found stone does not settle
Finding a stone is the easy part; knowing what it means is harder. Gallstones are common enough that many a patient carries them in silence for a lifetime; a stone found in someone whose pain has another source is a bystander, the scan that names it answering a smaller question than the one asked. A stone seen in a patient whose pain fits the gallbladder points the finger; the same stone in a patient whose pain is elsewhere is a finding to note and set aside, the clinical picture deciding which it is.
The bedside scan settles presence, though not always its meaning. It can say with confidence that stones are there, that the gallbladder is packed or clear, that a lump is a stone or a polyp; it cannot on its own say that those stones are the reason a patient hurts, nor clear the bile duct beyond the gallbladder. Read as a finder of stones and a sorter of their mimics, the handheld is a fast and certain tool; pushed to explain every pain it meets, it overreaches; the wider workup is what closes the gap between a stone seen and a diagnosis made.
The probe and the stone
Gallstones are the cleanest call the abdominal probe makes and one of its great satisfactions, the bright focus with its sharp shadow rolling downhill on cue a sign reliable enough that a confident diagnosis takes seconds at the bedside. The skill lies less in finding the obvious stone than in the edges around it: the gallbladder packed tight enough to hide inside its own shadow, the small stone too faint to shadow, the polyp that holds still, the stone in the neck that turns an idle gallbladder dangerous, the stone found that explains nothing. A clinician who knows the three marks of a stone and the handful of mimics that fake one of them carries in one hand a quick answer to one of the commonest questions the belly asks, as long as the stone is read for what it is, a finding to be weighed against the patient instead of taken as a diagnosis on its own. The stone seen clearly, sorted from its mimics, handed to the clinical picture for its meaning; that is the whole of what the bedside owes the question.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.