How Phone Ultrasound Works With Wireless Probe and Smartphone
A phone ultrasound looks like magic at the bedside. A clinician holds a small probe against the skin. A picture of the body appears on an ordinary phone. There is no cart, no cable to a console, no separate screen. The magic is engineering, and the engineering rewards understanding. A clinician who knows how the picture reaches the phone reads its quirks instead of fighting them.
The system has three parts.
There is the probe, which makes and reads the sound. There is the link, which carries the picture. There is the phone, which shows it and runs the controls. Each part does one job. Follow the signal through all three, and the whole device stops being a black box.
What the probe does
The picture on the phone is the last step of a chain that starts inside the probe and ends in the palm.
The probe is the machine. On a phone ultrasound, the part the clinician holds is not a dumb sensor on a wire. It is a complete scanner. Four parts share the housing. The transducer sends and receives sound. The electronics shape the beam. A processor turns echoes into an image. A battery powers it all.
The phone is the screen. The brain sits in the probe.
This split matters. It deserves a full look. It explains nearly every behaviour of a phone ultrasound that puzzles a new user. Sound is the tool. The probe sends a pulse of ultrasound into the body, far above the pitch a human ear can hear. The pulse travels until it meets a boundary between tissues, where part of it reflects back. The probe falls silent and listens for that echo. It times how long the echo takes to return, since a later echo came from deeper inside. It measures how strong the echo is, since a brighter echo marks a sharper boundary. From thousands of these pulses, fired in a fan across the region of interest, the processor inside the probe builds a single grey picture. Brightness stands for echo strength. Position stands for depth and direction. All of this happens in the handpiece, dozens of times a second, before anything reaches the phone. The probe has already done the hard work of imaging by the time a picture exists to send. That is why a phone ultrasound drains its own battery. The handpiece warms during a scan. Its price sits closer to a medical device than to an accessory. The intelligence that once filled a cabinet now sits in the grip of a hand. The phone, for all its power, only displays what the probe has already made.
How the picture reaches the phone
The link is the bridge. A finished image has to travel from the probe to the phone. Two paths exist. A wired probe plugs into the phone’s port and sends the picture down the cable. A wireless probe sends it over a radio link, the way a pair of headphones receives sound.
The wireless path is the harder trick.
A live scan is a stream of images, many every second. Each one has to arrive whole. It has to arrive in order. It has to arrive fast enough that the picture keeps pace with the probe in the hand. A delay of even a fraction of a second would break the link between what the hand does and what the eye sees. So a wireless probe leans on a dedicated radio channel. The link is often a private dual-band one, away from the crowded channel a home shares with its neighbours. It compresses each image to fit the channel. It accepts a tiny, steady delay in trade for a picture that does not stutter. These choices are why a wireless probe pairs the way it does, and why it asks the clinic to keep the phone close.
What the phone adds
The phone is the face of the system. It shows the picture. It carries the controls a clinician taps to change depth, brightness, or mode. It stores the study. It sends the study onward. The app on the phone is the dashboard, and the probe is the engine beneath it.
The phone also lends its strengths.
A modern phone has a bright screen. It has a fast processor. It has a network connection. It has a camera. A phone ultrasound borrows all of them. The bright screen shows the scan in clinic light. The processor runs the guidance software that coaches a user toward a standard view. The network sends a study to a colleague or the records system. The phone the clinic already owns becomes the console the cart used to be, at none of the cart’s bulk. The probe supplies the medicine. The phone supplies the convenience.
Why compatibility is not automatic
A phone ultrasound ties two devices together. The two have to agree. A probe built to pair with one family of phones may refuse another. The app may run on a current model and drop an older one. The clinic that owns a mix of handsets has to check each against the probe’s support list.
Check the list before the purchase, never after.
The reason sits in the link and the app. A wired probe needs the right physical port and the right data path through it. A wireless probe needs a radio the phone supports and an app the phone’s operating system still runs. A phone a year past the support window can leave a working probe with nothing to talk to. The hardware in the hand may be sound. The handset it was meant to pair with decides whether it works at all.
The quirks the design explains
Once the three parts are clear, the device’s habits make sense. The probe warms, since the imaging happens inside it. The phone stays cool. The battery in the probe drains, since it powers the scan and the transmission together. The picture lags by a hair because the wireless link trades a little delay for a steady stream. The app sometimes asks the phone to stay near the probe, since the radio link is short by design.
None of these are faults. They are the cost of the architecture.
A clinician who reads them as faults grows frustrated and blames the device. One who reads them as the natural price of a scanner that fits in a pocket works around them with ease. Keep the probe charged. Keep the phone close. Expect a little warmth on a long scan. Treat the picture as the probe’s work, shown on the phone, and the system behaves exactly as its design intends.
Reading the grey picture
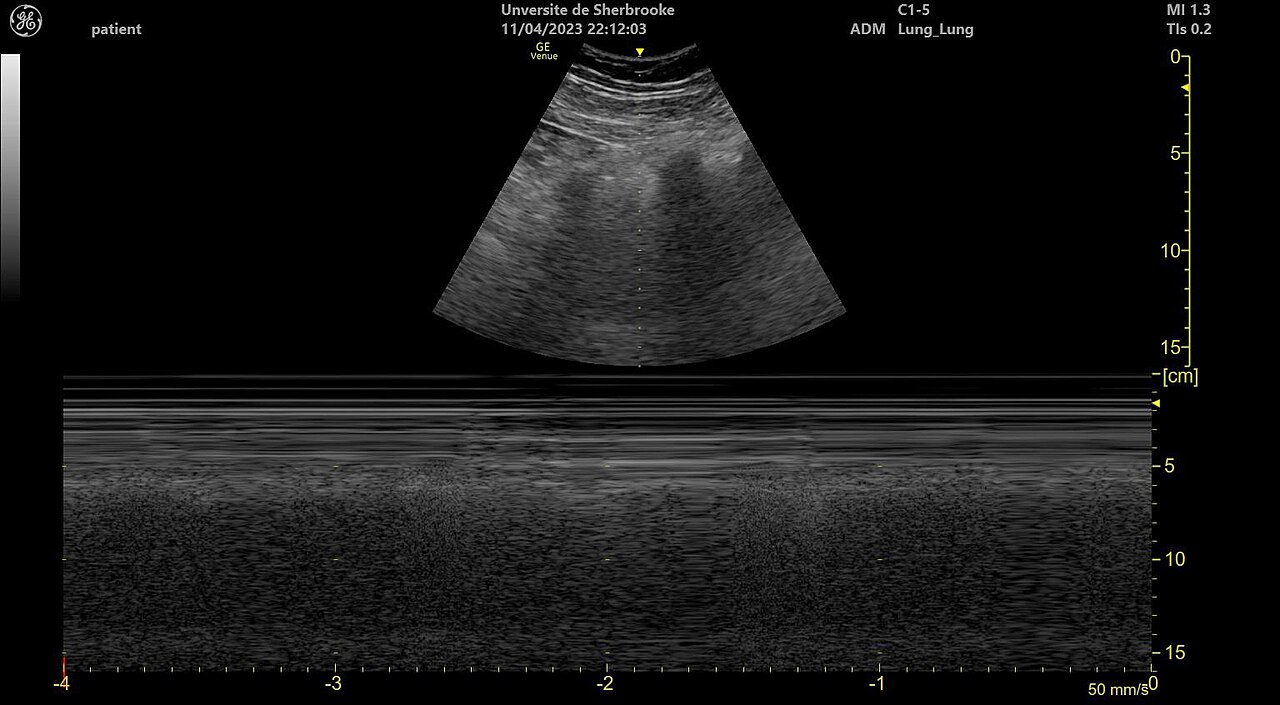
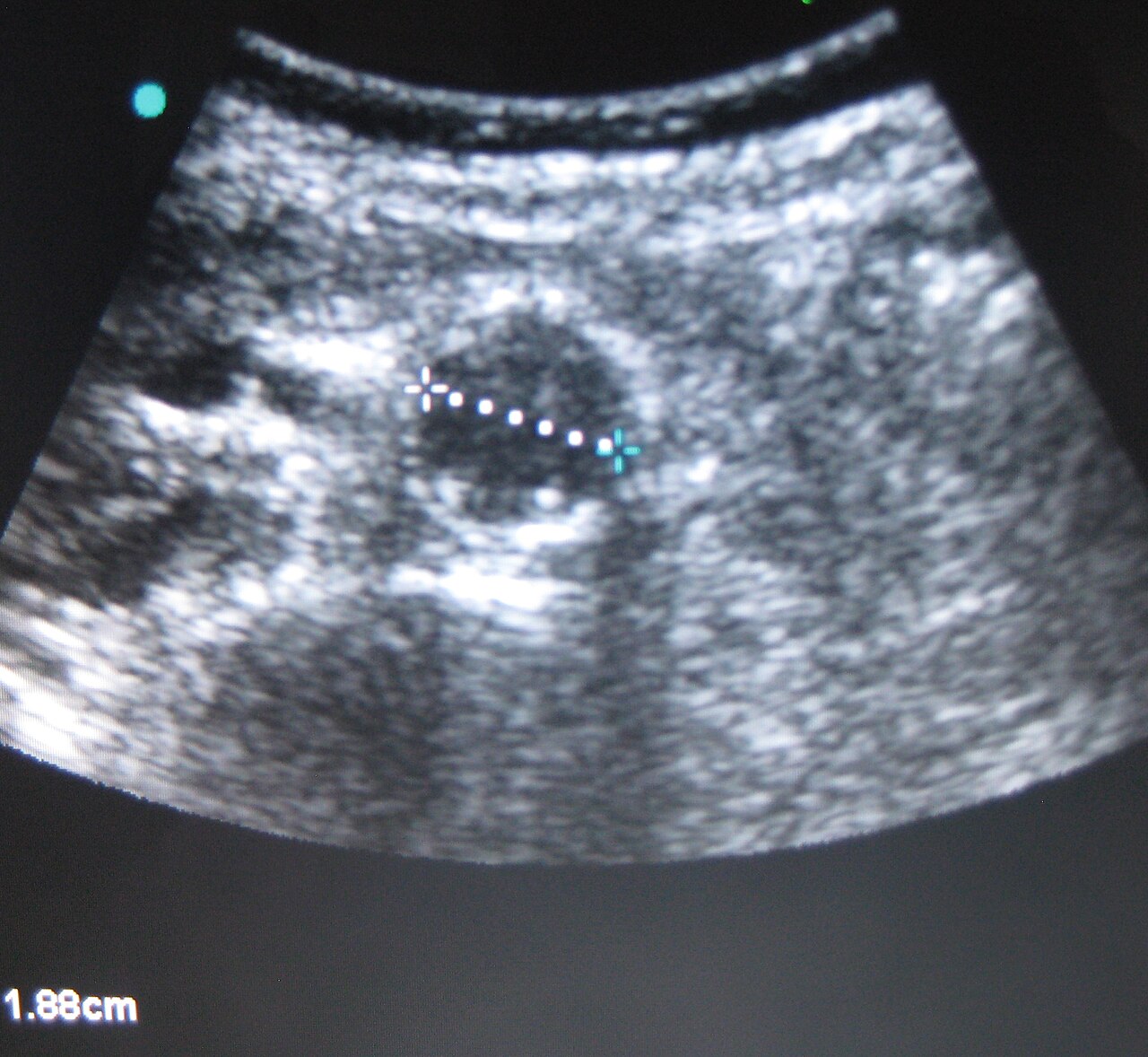
A clean cross-section like this is the output of dozens of focused beams assembled into one frame.
The image on the phone is grey for a plain reason. Ultrasound carries no colour of its own. The probe measures one thing about each echo: its strength. Strong echoes paint white. Weak echoes paint dark grey. Fluid sends almost nothing back. It paints black. A clinician reading the screen is reading a map of echo strength, nothing more.
Depth runs down the screen.
The top of the image sits just under the probe face. The bottom sits deep in the body. A structure low on the screen lies far from the skin. The width of the picture is the fan of the beam, sweeping side to side. Learn those two axes, and the flat grey image turns into a slice through the body, read at a glance. The skill takes practice. The layout never changes, so the practice pays off fast.
Artifacts ride along with the method. Sound that bounces twice can paint a structure that is not present. Gas throws a shadow that hides what lies behind it. Bone stops the beam dead and leaves a dark stripe below. A clinician who knows these tricks reads past them. One who does not mistakes an artifact for a finding. The probe reports its echoes honestly. Sorting the real from the false is the skill the device cannot supply.
Keeping the wireless link healthy
A wireless link is a quiet dependency. It works until something crowds it. The radio band a probe uses is shared. Other devices, thick walls, a body between probe and phone: each can thin the signal. A thinned signal shows as a stutter in the picture or a longer lag between hand and image.
Keep the phone within arm’s reach of the probe.
The fix is rarely technical. Move the phone closer. Set it where no body blocks the path. Keep the probe charged, since a low battery weakens the radio along with the scan. A clinic that treats the link as fragile, then handles it gently, rarely meets a problem. One that leaves the phone across the room blames the device for a fault of distance. The link was built short on purpose. Respect that, and it holds steady through a full exam.
When the phone is the weak link
The probe does the medicine. The phone can still let it down. An old handset with a dim screen hides detail a clinic light would already wash out. A slow phone stutters on the guidance software the probe leans on. A phone with a full storage drive refuses to save a study. The probe scanned well. The phone failed to show or keep the result.
Match the phone to the probe, not the other way round.
A clinic that pairs a capable probe with a tired phone wastes half of what it paid for. The screen sets the detail a clinician sees. The processor sets how smoothly the picture and the guidance run. The storage sets whether a study survives. A clean, current handset, kept charged and clear of clutter, lets the probe show its full picture. The cheapest path is a good probe on a good phone, since a good probe on a poor phone scans into a window too small to use.
Why it costs what it costs
The price of a phone ultrasound surprises people. The thing in the hand is small. The number on the invoice is not. The surprise fades once the architecture is clear. The clinic is buying a complete scanner, shrunk into a handpiece. The beamformer that once filled a cabinet now sits in the grip. The cost of that engineering did not vanish. It moved into the probe.
The phone is the cheap part. The probe is the device.
A buyer who reads the price as the cost of a phone accessory reads it wrong. The phone is borrowed. The medicine sits in the probe, in the array, the chip, the firmware, the clearance that lets it touch a patient. A clinic that grasps this stops comparing a medical probe to a gadget. It compares the probe to other scanners, judged on the picture it makes and the years it lasts. Read against that, the price tells a fairer story than the small size of the object suggests.
Putting it together at the bedside
The whole sequence runs in a heartbeat. The clinician sets the probe on the skin. The probe fires its pulses, listens for the echoes, builds a picture, and sends it across the link. The phone shows the picture, takes the taps that adjust it, and holds the study for the record. Three parts, one motion, a picture of the inside of a body on a device that fits in a coat pocket.
The magic was never magic.
It is a scanner shrunk into a handpiece, a radio link borrowed from consumer electronics, and a phone pressed into service as a screen. Understanding the three parts turns a mysterious gadget into a tool a clinician trusts. The picture comes from the probe. The link carries it. The phone shows it. A device understood this way is a device used well. A clinic that grasps the chain spends its attention on the patient, with the machine all but forgotten in the hand. That trust, once earned, turns a clever object into plain routine care, the kind a clinician reaches for without a second thought.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.