Three thousand dollars buys a real ultrasound machine now. A decade ago it bought nothing of the sort. The figure marks the line where a personal scanner moved from a hospital purchase to something a single clinician, a small clinic, a trainee could own. What that money buys, and what it leaves out, is the whole subject here.
The price fell as the machine shrank.
A scanner that fits in a pocket needs no console, no cart, no large screen. The cost of all that vanished from the bill. What remains is the probe itself, the part that does the imaging, plus the software that drives it. Under three thousand dollars, the buyer is paying for that core, and little else.
What the money buys
A personal scanner under three thousand dollars is, in nearly every case, a single handheld probe. It pairs with a phone or tablet the buyer already owns. It carries one transducer, tuned for one kind of work. It runs the basic imaging modes a focused exam needs. That is the shape of the device at this price. One probe, one job. The single probe is the heart of the trade. A curved probe at this price reaches deep, for the abdomen or a pregnancy. A linear probe stays shallow and sharp, for vessels or a thyroid. A phased-array probe reads the heart. The buyer picks the one that matches the work. A device that tries to cover every probe in one head, at this price, usually does each job a shade worse than a dedicated probe would.
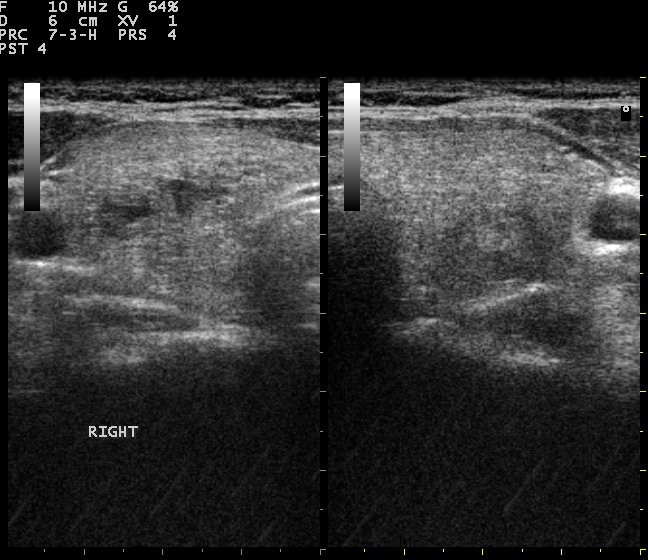
The picture a personal probe makes, shown on a phone the buyer already owns. (Nevit Dilmen (talk), CC BY-SA 3.0, via Wikimedia Commons)
What drives the price
The number on the invoice is not arbitrary, and it pays to understand what sits behind it, since the same three thousand dollars buys different machines depending on where a maker spent it. The largest cost is the transducer, the array of tiny elements that send and receive sound. A finer array, with more elements and cleaner electronics, draws a sharper picture and costs more to build. The second cost is the beamformer chip, the silicon that times the array and assembles the echoes. A more capable chip reaches more frequencies, runs more modes, and lifts the price. The third cost is the software, the part that turns raw echoes into a usable image and guides the user through an exam. Good software is expensive to write and to keep current, and a maker that invests in it charges for it. The fourth cost hides from the buyer entirely: the clearance that lets the device touch a patient legally, the testing behind it, the support structure that answers when a probe faults. A device priced well under three thousand dollars has saved money somewhere on this list. The skill of buying at this price is reading which corner the maker cut. A cheaper array means a softer picture. A weaker chip means fewer modes. Thin software means a clumsy exam. A missing clearance means a legal risk dressed as a bargain. The same listed price can hide a fine probe with a thin warranty or a crude probe with a generous one. Two identical figures buy two different bets on the years ahead. The price is a sum of these parts. A buyer who knows the parts reads the number for what it truly says about the device behind it.
Cheap is never free. It is a choice about where to save.
New versus refurbished
Three thousand dollars buys a new entry device. It also buys a refurbished higher one. The choice splits buyers. A new budget probe arrives fresh, under full warranty, with the maker behind it. A refurbished premium probe offers a better picture for the same money, with a shorter warranty and a longer history. Each path carries its own risk.
The new budget device is honest about what it is. The refurbished premium one tempts with a sharper image. Its battery has aged. Its probe face has worn. Its support may have lapsed with the original owner. A buyer drawn to the refurbished route checks the battery health, the warranty that remains, and the maker’s willingness to support a second owner. Bought with eyes open, a refurbished probe can be a fine deal. Bought on the picture alone, it can become an orphan the moment it faults.
Where the savings hide their cost
A low price often borrows from the future. The probe that costs little to buy can cost much to keep. A battery that ages fast, a probe face that cracks under harsh cleaning, a maker that charges heavily for a replacement: each turns a cheap purchase into a dear one over a year or two. Read the running cost. The sticker tells half the story. Ask what a replacement probe costs, since on a single-probe device the probe is the whole machine. Ask how long the warranty runs, and what it covers. Ask whether the software keeps getting updates, or stops the day the next model ships. A device that is cheap to buy and dear to keep is no bargain. One that costs a little more, then runs for years on a living warranty and fresh software, often spends less in the end.
The trap of the lowest listing
A search for a cheap ultrasound probe returns a wall of numbers. The lowest one tempts hardest. It is also the one to study with the closest care. A price far below the rest is rarely a gift. It is a signal. The cheapest listing usually hides the biggest gap.
A probe priced at a fraction of its peers has saved money somewhere a buyer cannot see in a photo. It may carry no clearance for the buyer’s market. It may ship from a seller with no support behind it. Its software may be a frozen build that the next phone update will break. Its warranty may exist on paper alone, honoured by a seller the buyer cannot reach. The picture in the listing looks fine, since a still image flatters every probe. The trouble surfaces later, on a patient, on a phone that updated, on the day a probe faults and the seller has vanished. A buyer who treats the lowest number as the best deal often pays twice: once for the cheap probe, again for the proper one that replaces it. The honest entry price has a floor. A listing far below that floor is selling something other than a working medical device.
What three thousand dollars cannot buy
Knowing the limits protects the buyer as much as knowing the strengths. Under three thousand dollars, a personal scanner will not match a hospital console on the hardest work. It will not read faint, deep flow in a large patient. It will not run the full suite of advanced cardiac or vascular modes. It carries one probe. It will not switch from a deep abdominal view to a shallow vascular one without a second purchase.
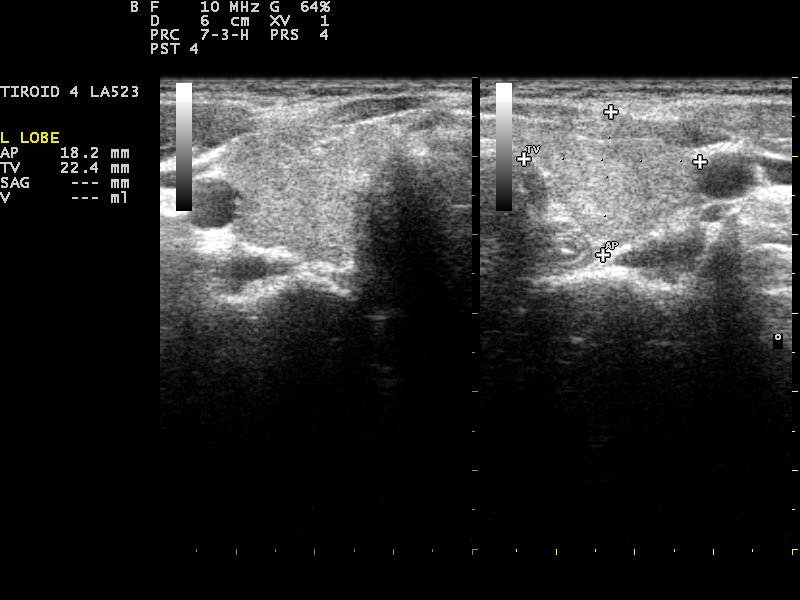
A focused image at this price answers a narrow question cleanly. (Nevit Dilmen (talk), CC BY-SA 3.0, via Wikimedia Commons)
It answers a focused question. It does not replace a department. A buyer who expects a console for the price of a laptop meets disappointment on the first hard scan. A buyer who expects a focused, portable tool, matched to one kind of work, meets a device that does exactly what it promised. The gap is one of expectation, not of fault. The price buys a real scanner for a real, narrow job. Asked to be more, it falls short, the way any tool does when pushed past the work it was built for. Naming the job before the purchase keeps the expectation honest, and the satisfaction high.
The phone is part of the cost
A personal scanner under three thousand dollars assumes a phone. The price does not include one. A buyer who reads the figure as the whole cost forgets the screen the probe needs to work. The probe is half a system. The phone or tablet is the other half. Its screen sets the detail a clinician sees. Its processor runs the app and the guidance. Its storage holds the studies. A capable probe on a dim, slow, full handset wastes much of what it cost. A buyer at this price should count the phone in the budget, or confirm the device runs well on the handset already owned. The cheapest path is a good probe on a phone that can show its picture. A good probe on a poor phone scans into a window too small to read, and the saving on the handset becomes a loss on the scan.
Who buys at this price
The under-three-thousand market serves people the old prices shut out. A trainee can own a probe to learn on. A rural doctor can carry imaging where no cart will go. A small clinic can keep a scanner at the bedside without a hospital budget. A specialist can add a focused tool to a practice for the price of a laptop. The low price changed who can scan.
This is the quiet importance of the price point. A scanner under three thousand dollars is not a worse hospital machine. It is a different thing entirely: a personal tool, owned by the clinician who uses it, carried to the patient, learned on at leisure. The price did not just shrink a budget. It put ultrasound in hands that never held it before, in places that never housed it. For the buyer the lesson is to judge the device by what that personal use needs, set against the specifications of a hospital console it was never meant to be.
How the price tracks the probe
The probe type sets a floor under the price. Not every probe costs the same to build. A buyer who knows the order avoids paying linear money for a curved job. The shape of the array drives the cost.
A curved probe, for deep abdominal work, uses a wide low-frequency array. A linear probe, for shallow sharp views, packs a dense high-frequency array into a flat face. A phased-array probe, for the heart, squeezes a small footprint between the ribs and leans hard on its electronics. Each design carries a different bill of materials. The same three thousand dollars stretches further on one type than another. A simple curved probe sits comfortably under the figure with room to spare. A fine linear probe, with its dense array, crowds the ceiling. A capable phased-array probe, asked to read a moving heart, pushes hardest of all against the limit.
A buyer shopping for a single type reads the price against that probe type, never against the cheapest probe on the page. A linear probe priced like a budget curved one has cut a corner the buyer will meet at depth. Matching the expected price to the probe the work needs keeps a buyer from mistaking a weak probe for a deal, or a fair price for a markup. The number means little until it is read against the kind of probe behind it. A clinic that names the probe first, then sets a fair price for that probe, walks into the market with a yardstick. A clinic that shops on the raw number alone walks in with none. It pays the difference later.
Buying well under three thousand
The decision comes down to a few honest questions. What single probe does the work need? Does the picture answer that work on a real patient? What does a replacement probe cost, and how long is it covered? Does the software keep current? Does the device carry the clearance the buyer’s country requires? Answer those, and the price tells the truth. A personal ultrasound under three thousand dollars rewards a buyer who knows the trade behind the number. The money buys one good probe, matched to one kind of work, on a phone the buyer already owns. It does not buy a hospital system, and it was never meant to. Bought against its real purpose, a personal scanner at this price earns its place, in a coat pocket, at a bedside, in the hands of someone who could never have owned one before the price came down to meet them.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.