The eFAST exam takes the trauma FAST and reaches into the chest. The plain FAST asks whether a patient is bleeding into the belly or the heart’s sac. The extended version adds the lungs, looking for two chest injuries that can kill as fast as a belly bleed: air in the pleural space, plus blood in it. The letter that turns FAST into eFAST stands for extended. The extension is the chest.
Same exam, two more questions.
A trauma patient does not bleed in one place by appointment. A blow that tears the spleen can also collapse a lung or fill a chest with blood. The eFAST checks all of it in one sweep, at the bedside, in the minutes a crashing patient allows. It adds the pleura to the FAST windows, using the same probe, the same speed, the same hunt for a finding that changes the next move.
What eFAST adds over FAST
The classic FAST looks at four spaces: the right flank, the left flank, the pelvis, and the heart. The eFAST keeps all four. It adds a look at the lungs on each side of the chest, high on the front for air, and lower on the flank for fluid. Two new questions join the four old ones. Air on top, blood below. Air, lighter than tissue, rises to the highest point of the chest in a patient lying flat. The probe hunts a collapsed lung on the front of the chest, near the breastbone. Blood, heavier, sinks. The probe hunts a bloody chest above the diaphragm, in the same flank windows the FAST already uses. The eFAST reads both with a small shift of the probe. The two findings need two different, urgent responses.
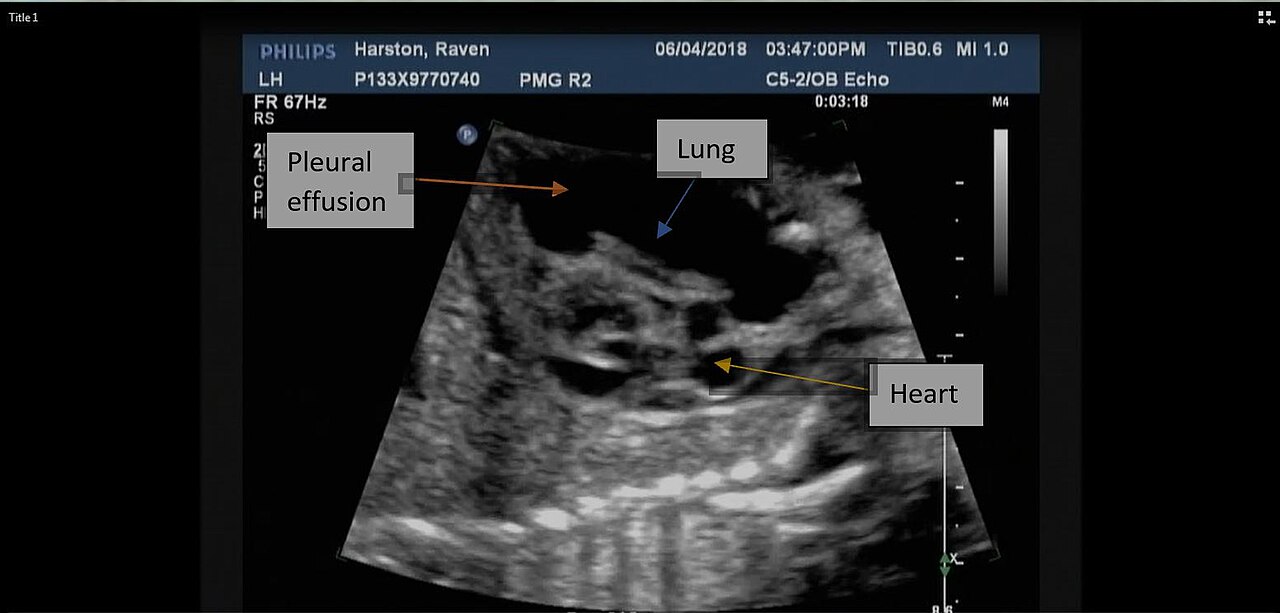
Fluid above the diaphragm reads as a dark space, a hemothorax on the chest view. (Harstonraven, CC BY-SA 4.0, via Wikimedia Commons)
Hunting a collapsed lung
The search for a collapsed lung, a pneumothorax, is the heart of what eFAST adds. It rewards a close look, since the sign it relies on is unlike anything else in trauma ultrasound. A normal lung, pressed against the chest wall, slides a little with every breath. The two layers of the pleura, the lining of the lung and the lining of the chest, glide over each other as the lung inflates and empties. On ultrasound this glide shows as a shimmer at the pleural line, a fine sparkle that moves with the breath. Clinicians call it lung sliding. When air leaks into the space between the two pleural layers, in a pneumothorax, it pushes them apart. The lung no longer touches the chest wall at that spot. The slide disappears. The pleural line goes still. The search for a pneumothorax becomes a search for absence: the absence of the slide that a healthy lung always shows. A clinician places the probe high on the front of the chest, where free air rises in a patient lying down, then watches the pleural line for the shimmer. Present, the lung is touching the wall there. A pneumothorax at that spot is ruled out. Absent, the slide is gone. A collapsed lung climbs to the top of the list. The reading is quick once the eye knows the shimmer. It carries a trap, though: the slide can be absent for reasons other than a pneumothorax, in a lung that is not moving air at all, and the sign is read as one clue among the patient’s whole picture. The surest finding is the lung point, the exact line where a sliding lung meets the still, collapsed region, a sign specific enough that its presence nearly confirms the diagnosis.
Absence is the finding here.
Hunting blood in the chest
The second new question is simpler. Is there blood in the chest, a hemothorax. The answer uses the same flank windows the FAST already scans, with the probe aimed a little higher, above the diaphragm instead of below it. Above the diaphragm is the chest. Below it is the belly.
The diaphragm shows on ultrasound as a bright curved line, with the liver or the spleen beneath it. In a healthy chest, the space above that line is filled with air-filled lung, which scatters the sound into a mirror-like grey. When blood collects above the diaphragm, it shows as a black space, the same dark fluid the FAST hunts in the belly, only one level up. A clinician who already scans the flanks for a belly bleed tilts the probe a touch higher and reads the chest above the diaphragm in the same motion. A black wedge there is blood in the chest, a hemothorax that may need a drain.
One sweep, six windows
The eFAST runs as one continuous exam. A clinician moves through the right flank, the left flank, the pelvis, the heart, then the two lung windows, in a fixed order, every time. The chest views fold into the route without adding much time. The whole sweep still takes only minutes. Order protects the exam under pressure. A clinician who runs the same six-window route on every trauma patient never forgets the chest in the rush to check the belly. The added lung views cost seconds. They catch two injuries the plain FAST would have missed. A patient with a quiet abdomen and a collapsing lung is found by the eFAST, missed by the FAST, which is the whole reason the extension exists.
Why the chest views matter
A tension pneumothorax kills by squeezing the heart and the great vessels as trapped air builds pressure in the chest. A large hemothorax kills by blood loss and by crowding the lung. Both can develop in a patient whose belly is dry. Both have a fast, definite treatment: a needle or a drain. The value of the chest views is that they catch these injuries early, with a tool already in the clinician’s hand. The treatment is fast once the finding is clear.
A pneumothorax under tension needs air let out, now. A hemothorax needs a drain and blood replaced. Neither waits well. The eFAST puts the finding in front of the clinician in the first minutes, before a chest film could be shot and read, before the patient is moved. A collapsing lung caught on the front of the chest, in the resuscitation bay, is a collapsing lung treated before it crowds the heart. That head start is the gift the chest views add to the trauma survey.
Setting up the lung views
The lung views reward a little care in setup. The probe choice is forgiving. A linear probe shows the pleural line in fine detail. A curved or phased probe, already in the clinician’s hand for the belly windows, reads the slide well enough. So the eFAST rarely needs a probe change between the abdomen and the chest. The patient lies flat. The air rises.
Position decides where to aim. In a patient on their back, free air climbs to the front of the chest, just below the breastbone. That is where the probe goes first. The clinician sets it between two ribs, finds the bright pleural line, then watches it through a breath. A doubt about the slide meets a second test. The clinician switches to M-mode, a tracing that turns motion over time into a pattern. A sliding lung draws a sandy, grainy band below the pleural line, the seashore sign. A still lung draws straight horizontal lines, the barcode sign. The two patterns are easy to tell apart, even when the live shimmer is hard to judge by eye. A clinician uncertain on the moving picture reaches for M-mode and lets the pattern settle the question. The setup is quick, the tests are few. Together they turn a subtle finding into a readable one.
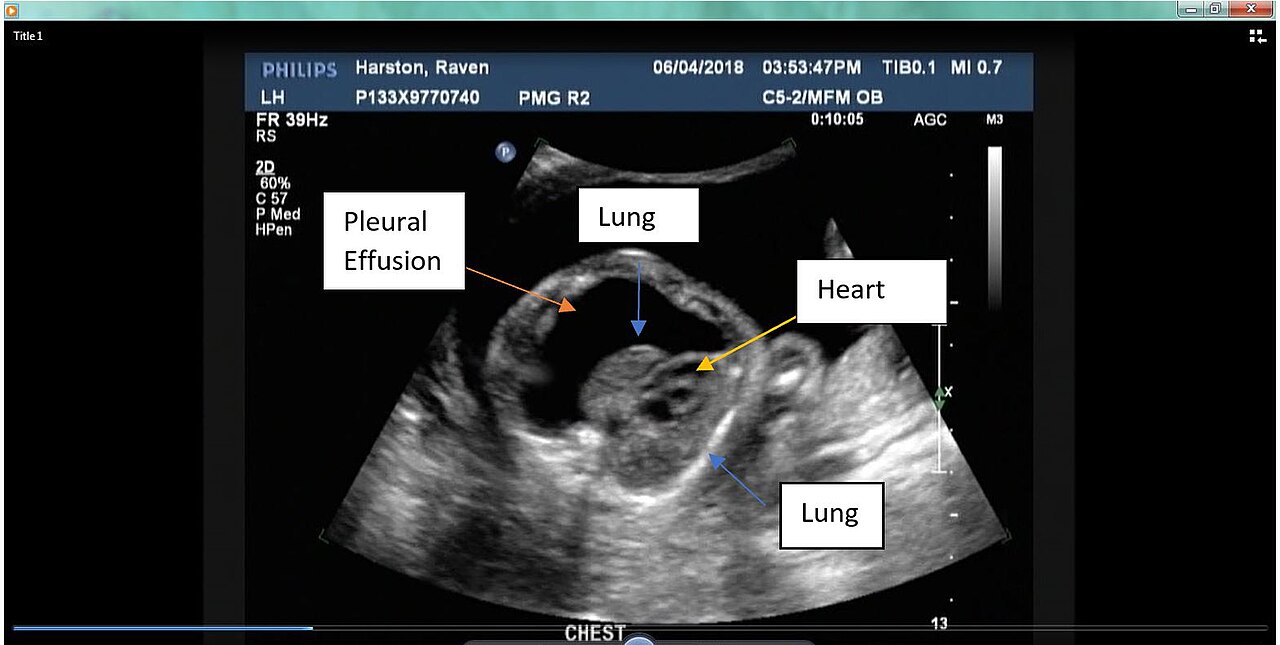
A pleural collection seen on a focused chest ultrasound. (Harstonraven, CC BY-SA 4.0, via Wikimedia Commons)
eFAST against the chest X-ray
For decades the chest X-ray was the first look for these injuries. The eFAST changed the order. The two tools answer the same questions, with different strengths. A trauma team uses both. Ultrasound is faster. The film is broader.
The eFAST reads a pneumothorax and a hemothorax at the bedside, in the first minute, before a patient is moved. A supine chest film, shot flat in the bay, can hide a small pneumothorax that lies against the front of the chest, the place ultrasound reads best. So for the urgent question of air in the chest, ultrasound often beats the film a flat patient can give. Against that, the X-ray shows the whole chest at once: the ribs, the great vessels, the position of a tube, findings the eFAST never sees. The two tools are partners more than rivals. The eFAST acts first, in the seconds a crashing patient allows. The film fills in the wider picture once the patient is stable enough to shoot a good one. A team that leans only on the film loses the speed of the bedside. A team that leans only on the ultrasound loses the breadth of the film. The trauma bay keeps both, and reaches for each when its strength fits the moment.
The traps in the chest views
The lung views are powerful and easy to misread. Absent lung sliding does not always mean a pneumothorax. A lung that is not ventilating, a patient holding their breath, a tube placed down one side only: each can still the slide without any air leak. A clinician reads absent sliding as a strong clue, well short of proof on its own.
A still pleural line has more than one cause.
The lung point settles the doubt when it appears, since it marks the exact edge of a collapse and points only to a pneumothorax. Subcutaneous air, trapped under the skin after an injury, can also wreck the view by scattering the sound before it reaches the lung. A clinician who knows these traps reads the chest views with care, weighs them against the patient’s breathing and injuries, and reaches for a chest film or a scan when the ultrasound is unclear. The skill of eFAST is the same as the skill of FAST: knowing what a sign means, and knowing what its absence does not.
Learning the eFAST
The eFAST is among the first scans a trauma clinician learns, and for good reason. The belly windows take a few hours to grasp. The chest views take a few more. The signs are bold rather than subtle: a black stripe, a shimmer present or gone. The signs are bold enough to teach fast.
A learner builds the belly half on the plain FAST, then adds the two lung windows. The lung slide, once the eye catches it, is hard to unsee. The seashore and barcode patterns on M-mode give a fallback the learner trusts while the live picture is still new. A teaching program puts a probe in every learner’s hand, since the cost of a pocket device lets a whole class scan at once. Within a short course a clinician runs the full six-window sweep without thinking, in the order that protects against a missed view. The eFAST is hard to master to the last subtle case. It is quick to learn to the level a crashing trauma patient needs, and that gap, between quick competence and slow mastery, is what makes it the workhorse of bedside trauma imaging.
Where eFAST sits in the trauma workup
The eFAST is a first look, never a final answer. It runs in the first minutes, beside the primary survey, as the team stabilises the patient. Its findings steer the immediate moves: a drain here, a trip to surgery there, a fuller scan for the patient who can wait. It buys decisions, not diagnoses. A positive eFAST acts at once. A collapsing lung is decompressed, a bleeding belly is sent toward surgery, a bloody chest is drained, often before any other imaging exists. A negative eFAST does not close the case. It clears the urgent questions, then hands the patient to the slower, fuller workup that catches what a bedside sweep cannot. Read this way, the eFAST is the trauma team’s first set of eyes inside the body, fast enough to act on, repeated as the patient changes, and trusted for exactly what it was built to find: the bleeding and the collapse that cannot wait.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.