Pneumothorax Rapid Diagnosis Using Handheld Lung Ultrasound
A patient crashes after a blow to the chest, or a ventilated patient’s oxygen drops without warning. Air has leaked into the space around a lung and begun to collapse it. The clock starts the moment it does. A tension pneumothorax can stop a heart in minutes, squeezing the chest from inside until the great veins cannot fill it. The probe answers the question faster than a film can be shot and read. Is the lung still touching the chest wall, or has air pushed it away.
Air rises. The probe waits there.
The finding is a strange one, since a pneumothorax shows itself by what stops. A healthy lung shimmers against the wall with every breath. Air in the way kills the shimmer. The hunt is for an absence, a stillness where there should be motion, a quiet line where a living lung should dance.
The air that hides
Air in the pleural space is hard to catch the old way. A patient flat on their back sends free air to the front of the chest, the highest point of a body lying down. A chest film shot supine looks straight through that anterior air, since the air lies as a thin sheet against the front wall where the beam passes through it without an edge to cast a shadow. A small anterior pneumothorax, plain on a scan, can vanish on a supine film. The injuries that cause it arrive in patients too unstable to sit up for the upright picture that would show it.
The film looks through it. The probe sees it.
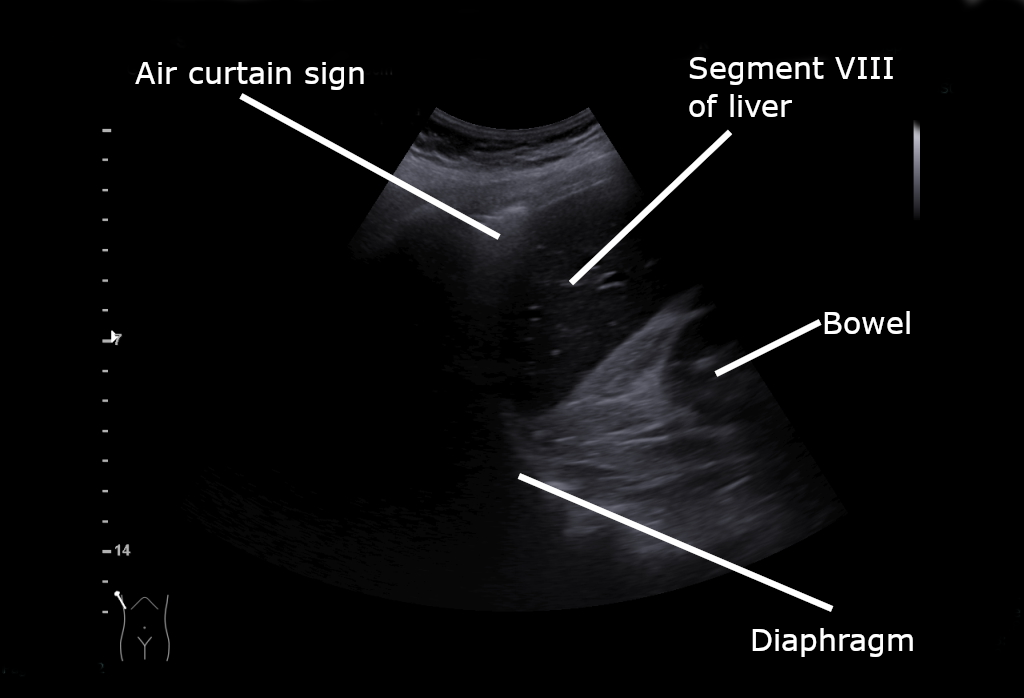
Normal lung: the bright pleural line with horizontal A-lines beneath. Wikimedia Commons, CC BY-SA 4.0
What the probe truly reads
Ultrasound and air are enemies, and that single fact is the whole basis of the exam. Sound cannot travel through gas. It scatters and dies at the first air it meets. A normal lung is full of air, which makes the lung itself invisible to the probe. Everything read at the chest is read at the pleural line, the bright stripe where the chest wall meets the lung, and almost everything seen below that line is an artifact, an echo of the probe’s own sound ringing in the tissue above. Two layers of pleura lie at that line. The parietal layer is fixed to the chest wall. The visceral layer is wrapped around the lung. In a healthy chest the two are pressed together, the visceral layer gliding against the parietal one with every breath as the lung inflates and empties. That glide is the one true motion the probe can see, a fine shimmer at the pleural line. The reverberation artifacts hang on the two layers staying in contact. Vertical beams called B-lines, when they appear, rise from the visceral pleura and need it touching the wall to form. A pneumothorax breaks the contact. Air slips between the two layers and drives the visceral pleura, with the lung behind it, away from the wall. The probe now reads only the parietal layer, still and alone. The shimmer is gone. The B-lines are gone. What remains is a set of flat horizontal lines, A-lines, the plain reverberation of the unmoving parietal pleura repeating down the screen. The missing slide is a sensitive sign, catching nearly every pneumothorax that sits under the probe, since interposed air reliably stills the visceral layer. It is far from specific. Anything that stops the visceral pleura from moving stills the slide too: a held breath, a lung fed by a tube passed down the wrong main bronchus, scarring that glues the layers, a stiff and diseased lung. The probe reads the stillness honestly. The clinician supplies the meaning.
The shimmer that rules it out
The exam begins with the shimmer. The clinician sets the probe high on the front of the chest, between two ribs, then finds the bright pleural line. A breath or two tells the story. A pleural line that shimmers, sliding back and forth as the patient breathes, means the two layers are touching at that spot. A lung touching the wall has no air wedged between it and the wall. A pneumothorax at that point is ruled out, plainly and at once.
The power of the sign sits in its certainty when present. A clear, lively slide is among the surest ways to exclude a pneumothorax at the spot under the probe, trusted enough that a confident shimmer ends the question there. The clinician lifts the probe, moves it a rib space along, asks the same question again, and builds a map of the chest one certain spot at a time.
The signs that also reassure
Two more findings carry the same weight. A B-line, the bright vertical beam that drops from the pleural line to the bottom of the screen, springs from the visceral pleura and forms only when that layer meets the wall. A single B-line at a spot rules out a pneumothorax there as firmly as the slide does. The lung pulse, a faint flicker of the pleural line in time with the heartbeat, says the same thing in its own way. The beat reaches the pleural line only when the lung is pressed against the wall to carry it.
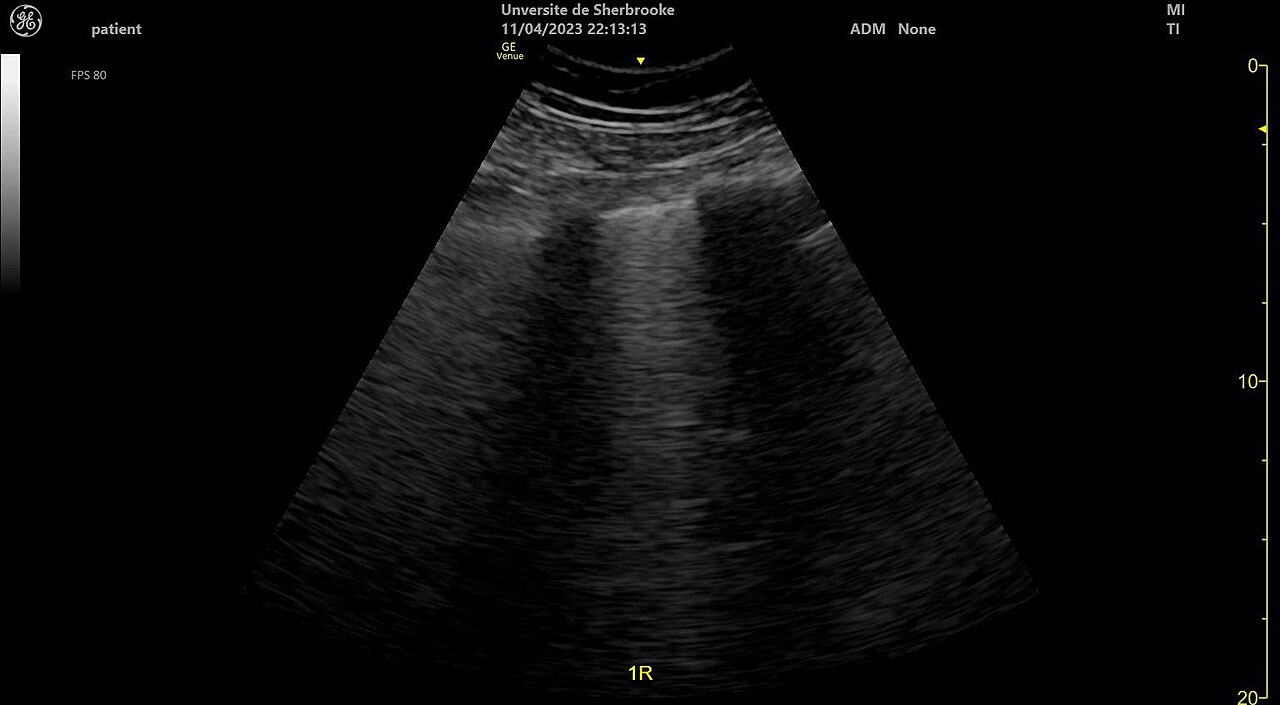
B-lines dropping from the pleural line; a single B-line at a spot also excludes a pneumothorax there. Wikimedia Commons, CC BY-SA 4.0
Any motion at the pleural line argues against air.
Seashore and barcode
When the live shimmer is hard to judge by eye, a second mode settles it. M-mode traces the motion of a single line of the image over time, drawing a picture of movement against stillness. Above the pleural line the fixed chest wall draws straight horizontal bands. Below it, a sliding lung stirs the tissue into a granular, sandy texture. The two together look like waves breaking on a beach, the seashore sign, and the sand below the line means the lung is moving against the wall. When the slide is gone, the sand turns to straight horizontal bands matching the still wall above. The whole tracing becomes a stack of parallel lines, the barcode sign, the signature of a pleural line that does not move at all.
The lung point
One sign stands above the rest for certainty. At the edge of a pneumothorax, where the collapsed lung still reaches the wall at the deepest part of a breath, the probe can catch the exact border between touching and not-touching lung. On the screen a stretch of sliding pleura sits beside a stretch of still pleura, and the boundary between them flickers in and out with each breath as the lung edge swells out to the wall, then falls back from it. That flicker is the lung point. It is specific enough that its presence nearly confirms a pneumothorax, since only a partial collapse produces a moving border of this kind. Its position maps the size of the collapse. A lung point found far around the side speaks of a large pneumothorax. One near the front speaks of a small one. A collapse complete enough that the lung never touches the wall has no lung point to find, a quiet trap for a clinician who reads its absence as an all-clear.
Absent sliding is a clue, never a verdict
The danger of the exam lives in the missing slide. A still pleural line is the finding that points at a pneumothorax, and it is the finding that lies more often than any other. A lung moving no air stills the slide with no leak at all. A breath held for the scan stills it. A tube passed down one main bronchus leaves the other lung motionless on the screen. Old scarring that glues the pleura together, a stiff diseased lung, a patch of deliberate pleurodesis: each stops the slide with the two layers still touching.
The defence is the one every focused exam needs. Absent sliding raises the question. The lung point answers it, when found. Read against the breathing, the history, the other windows, a still pleural line is a strong clue. Read alone, it sends a clinician chasing air that was never there.
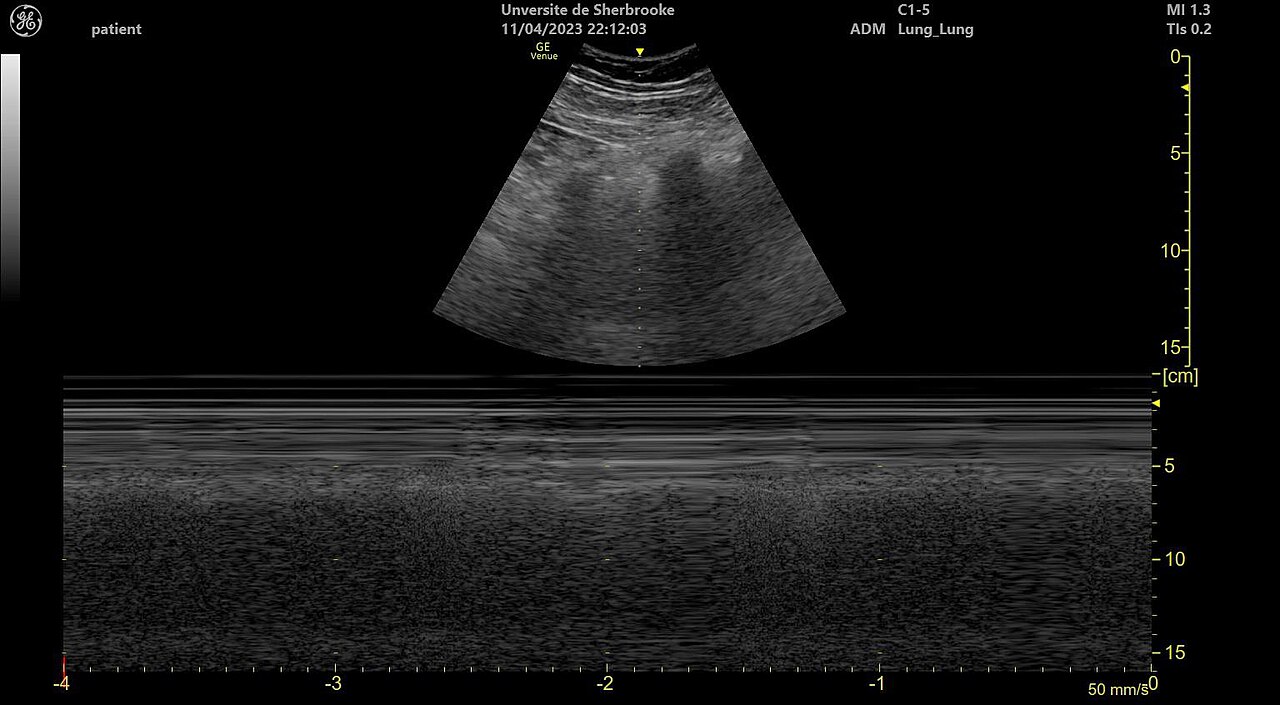
The seashore sign on M-mode: a sliding lung stirs the tissue below the pleural line. Wikimedia Commons, CC BY-SA 4.0
Where to aim
Position decides what the probe finds. A patient on their back sends free air to the front of the chest. The probe goes there first, high and near the breastbone, the place a small pneumothorax hides. From there the clinician works down the side, rib space by rib space, mapping how far the absent slide reaches across the chest. The lung point, where it exists, sits somewhere along that path, and finding it both confirms the diagnosis and measures its spread.
Air rises to the top. Scan the top first.
Against the chest film
The chest film and the probe answer the same question with opposite strengths. Ultrasound is the faster of the two, reading the front of the chest at the bedside in the first minute, before a film is shot and developed. For the anterior air a supine patient hides, the probe is the more sensitive, catching small collections the flat film looks straight through. The film answers a wider question. It shows the whole chest in one frame: the lung fields, the ribs, the great vessels, the position of a tube, the findings the narrow lung windows never reach.
A team keeps both. The probe acts first, in the seconds a crashing patient allows. The film fills the wider picture once the patient holds still enough to shoot a clean one. Each tool is reached for where its strength fits the moment.
The traps
Air outside the lung can wreck the exam as surely as air inside. After an injury, gas can track under the skin of the chest, a crackling layer between the probe and the pleura. That subcutaneous air scatters the sound before it reaches the lung, blanking the pleural line and every sign it would have carried. A clinician who meets a chest that gives no readable pleural line at all suspects air in the wall, a finding that points toward injury beneath instead of away from it.
The other trap is the eager eye. A clinician certain that a still line means a pneumothorax will find one where a held breath or a quiet lung is the real cause. The cure is the lung point and the patient’s whole picture, never the still line standing alone.
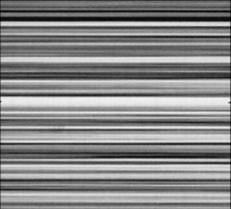
The barcode sign: a still pleural line draws only parallel lines, the mark of absent sliding. Wikimedia Commons, public domain
Scanning again as it changes
One scan is a frozen moment. A pneumothorax grows. A small leak caught early can become a tension hours later as more air escapes with each breath that finds the hole. A patient on a ventilator, pushed by the machine, can turn a trickle into a crisis fast. Repeating the scan as the oxygen or the airway pressure drifts catches the collapse before it grows past a simple drain.
Learning it
The exam is quick to reach a useful level. The slide, once the eye catches its shimmer, is hard to mistake. The seashore and barcode patterns give a fallback the learner leans on as the live picture is still new. A black-and-white answer at each spot, sliding or still, builds confidence fast across a short course. The lung point and the long list of mimics take longer to master, the part that separates a safe reading from a hasty one, the hours at the probe that turn a bold sign into a trustworthy one.
The slide is easy. Its absence takes judgement to read.
What it changed
Before the probe, an anterior pneumothorax in a supine trauma patient was a diagnosis the film often missed and the clinician found late, sometimes only when a chest was opened or a tension announced itself with a crashing pressure. Ultrasound put the pleura on a screen. The same handheld carried for the trauma survey reads the lung in the seconds between the belly windows and the next decision, in the bay, before any other imaging exists.
The deeper gift is a clear order among the signs. A slide, a B-line, a lung pulse: any one of them ends the question at that spot. A still line raises the question. A lung point settles it. A clinician who holds that order in mind reads a crashing chest fast, and treats the collapse that cannot wait, reaching it before an arrest.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.