The FAST exam asks one question of a trauma patient: is there free fluid where there should be none. In a crash victim, that fluid is blood. The exam looks in four places blood collects first, reads each in seconds, then gives a clinician an answer at the trolley as the team works. FAST stands for Focused Assessment with Sonography in Trauma. The name describes the discipline: focused, fast, aimed at one finding.
Four windows, one question.
The protocol is a fixed route through four views. Each window looks at a space where blood pools when an organ bleeds. A clinician runs the route in the same order every time. Nothing is missed under pressure. The four are the right upper quadrant, the left upper quadrant, the pelvis, and the heart.
Free fluid reads as a dark stripe where solid tissue should show grey. (Ben Smith, CC BY-SA 4.0, via Wikimedia Commons)
Why free fluid is the whole point
Blood obeys gravity. When an organ tears inside the abdomen, the blood does not stay put. It runs downhill, into the lowest spaces a lying patient offers. It pools there. The FAST exam works on a simple fact: those low spaces are few, known, easy to reach with a probe. Find fluid in them. The patient is bleeding inside. Fluid is black on the screen. Ultrasound paints blood and other fluid as black. Fluid sends almost no echo back. A solid organ shows as grey texture. A stripe or pocket of black where the screen should show only grey is the finding the whole exam hunts for. The eye learns it fast. A clinician new to FAST can spot a black stripe of free fluid within an afternoon of teaching.
The first window: the right upper quadrant
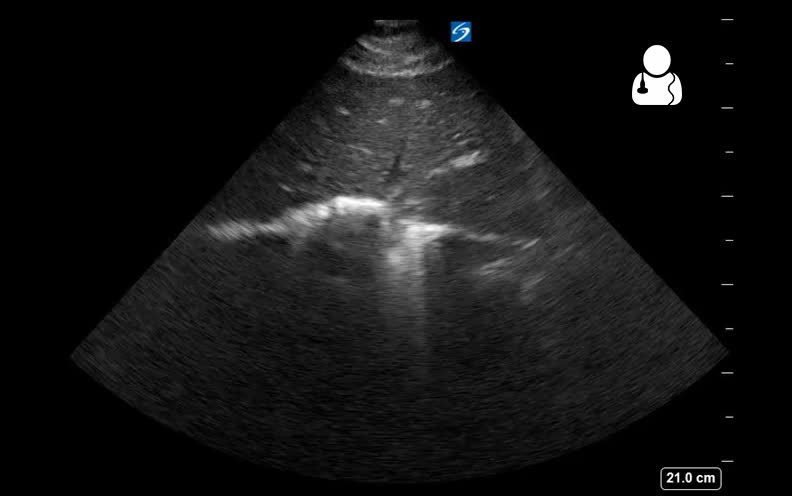
The right upper quadrant is the richest window, and it deserves a close look, since it catches more free fluid than any other view and is the first place a careful clinician checks. The probe sits on the right flank, between the lower ribs, aimed across the body. It shows the liver as a large grey organ, the right kidney tucked beneath it, and the line where the two meet. That line is the place to watch. The space between the liver and the kidney, called the hepatorenal recess or Morrison’s pouch, is the lowest point of the upper abdomen in a patient lying on their back. Blood from almost anywhere in the belly drains toward it under gravity. A small bleed shows here before it shows anywhere else. A clinician reads this view by looking for a black stripe in that line between liver and kidney, where healthy tissue shows only the two grey organs pressed together. The stripe can be thin, a few millimetres, in an early bleed, or thick and obvious in a heavy one. A clinician learns the look of that line empty before ever trusting the look of it full, since a new dark stripe declares itself only against a picture the eye already knows cold. The same window also catches fluid above the liver, against the diaphragm, and in the space below the lung at the top of the image. A clinician who learns to read this one view well catches the larger share of positive FAST exams, which is why the right upper quadrant is taught first, scanned first, trusted above the rest. A negative right upper quadrant does not rule out bleeding on its own, and a positive one, in a patient who is unstable, is often enough to send them straight to the operating room.
This window alone finds the larger share positives.
The second window: the left upper quadrant
The left upper quadrant mirrors the right, with a twist. The probe moves to the left flank, higher and further back than instinct suggests. It shows the spleen, the left kidney, and the spaces around them. The spleen is a common source of bleeding after a blow to the left side. This window matters in its own right. Aim higher and more posterior than feels natural.
The classic error is placing the probe too low and too far forward, where the ribs and the stomach gas hide the view. The fluid here collects above the spleen, between it and the diaphragm, more often than below it. A clinician reads the space around the spleen and the line between spleen and kidney, hunting the same black stripe. The left side is harder than the right. The spleen is smaller and higher than the liver, and the view is easily lost. Patience and a posterior probe win it.
The third window: the pelvis
The pelvis is the lowest space of all. In a patient lying flat, fluid that does not pool in the upper abdomen runs down here. The probe sits just above the pubic bone, aimed down into the pelvis, with the bladder as the landmark. A full bladder makes the view easy. An empty one makes it hard. The bladder is the window’s anchor. Behind and around the bladder lie the spaces where pelvic free fluid collects. In a reclining patient, blood pools here as readily as in Morrison’s pouch. A clinician scans the bladder in two planes, across and along, then looks for black pockets behind and beside it. The full bladder acts as an acoustic window, letting the sound pass cleanly into the pelvis. A clinic that can fill a stable patient’s bladder before the scan reads this window far more easily than one scanning a patient who has just emptied it.
The fourth window: the heart
The last window leaves the abdomen for the chest. The probe sits below the breastbone, aimed up at the heart, or beside the sternum if that view fails. It asks a different question. Is there blood in the sac around the heart, the pericardium, pressing the heart closed. Here the fluid can kill in minutes.
A bleed into the pericardial sac squeezes the heart until it cannot fill, a state that turns fatal fast. The FAST exam adds this window since a trauma patient can bleed into the chest as well as the belly, and the pericardial bleed needs a different, faster response. A clinician reads a black rim around the beating heart as the sign. The cardiac window also lets the clinician judge whether the heart is filling and squeezing at all, a clue to how much blood the patient has lost. The window is brief. Its answer can redirect the whole resuscitation.
The hepatorenal recess, where blood pools first in a supine patient. (Nevit Dilmen (talk), CC BY-SA 3.0, via Wikimedia Commons)
Running the protocol under pressure
The four windows are scanned in a set order, every time. Order is the protocol’s defence against a missed view in a chaotic room. A clinician who always runs right upper quadrant, then left, then pelvis, then heart, never forgets a window when the patient is crashing and the team is shouting.
The whole exam takes a couple of minutes. Speed is the point. A FAST exam is not a careful survey. It is a fast sweep for one finding, run as other care continues. A positive exam in an unstable patient sends them toward surgery without waiting for slower imaging. A negative exam buys time for a fuller scan in a patient who can wait. The clinician repeats the FAST as the patient’s state changes, since a bleed that was too small to see at first can grow large enough to find a few minutes later.
Setting the probe and the patient
A good FAST starts before the first image. The probe matters. A curved low-frequency probe reaches the depth the abdomen needs. It is the standard choice for the four windows. The patient matters more. A patient lying flat on their back sends fluid to the spaces the FAST checks. That position is the one the exam assumes. Position decides what the probe can find.
Tilting the patient changes where the blood pools. A slight head-down tilt drives fluid toward the upper abdomen, sharpening Morrison’s pouch. A head-up tilt drives it toward the pelvis. A clinician who knows this uses gravity as a tool, tilting a stable patient to bring a suspected bleed into a window. The probe pressure matters too. Heavy pressure flattens a thin stripe of fluid out of view. A light hand keeps it visible. The small choices of probe, position, and pressure separate a FAST that finds a subtle bleed from one that misses it. They cost nothing but the knowing.
When to scan again
A single FAST is a snapshot. A bleed is a moving thing. The exam read once, early, can miss a slow bleed that is still too small to see. The answer is to scan again. A repeated FAST catches the bleed that grows.
A clinician who runs a FAST on arrival, then again as the patient’s pressure or pulse shifts, watches the abdomen fill in real time. A stripe absent at first can appear minutes later as blood accumulates. This serial scanning turns the FAST from a single yes-or-no into a trend. A patient whose FAST stays clear through a stable hour is reassured in a way one snapshot cannot give. A patient whose FAST turns positive on a repeat scan declares a bleed that the first look missed. The exam costs a couple of minutes and no contrast, no radiation, no transfer, and a clinician can repeat it freely, as often as the patient’s course demands. The power of FAST is not only the first scan. It is the ease of the next one.
What the FAST cannot do
The exam is powerful and narrow. It finds free fluid. It does not find the source. It does not measure how fast a patient is bleeding. It misses bleeding behind the abdominal lining, in the space the FAST windows do not reach. A clear FAST is not a promise of safety.
A focused view used to read fluid and the beating heart. (Nevit Dilmen (talk), CC BY-SA 3.0, via Wikimedia Commons)
A negative scan rules little out on its own.
A small bleed can hide below the exam’s threshold. A retroperitoneal bleed sits outside its windows entirely. So a clinician reads a negative FAST as one input among several, weighed beside the patient’s pressure, pulse, and injuries, never as an all-clear. The exam earns its place by catching the bleeds that need surgery now, fast enough to act on. Asked to rule out every injury, it falls short, the way any focused tool does when pushed past the question it was built to answer. The skill of FAST is knowing both what a black stripe means and what an empty screen does not.
Reading a positive scan
A positive FAST is a black stripe where grey should be. The reading is binary at heart: fluid, or no fluid. The amount matters less than the presence. Even a thin stripe, in an unstable patient, points toward the operating room. Presence beats measurement here.
A clinician does not pause to measure a bleed on FAST. The exam was never built for that. It answers yes or no. The answer drives the next move. A thick band of black in a crashing patient confirms what the vital signs already screamed. A thin one in the same patient carries nearly the same weight, since a small visible bleed in someone whose pressure is falling is rarely the whole story. The exam hands the team a fact: there is blood inside. What to do with that fact belongs to the wider picture of the patient, not to the width of the stripe.
Why FAST built the field
The FAST exam was the application that proved bedside ultrasound to a sceptical profession. It answered a life-or-death question faster than a trip to the scanner allowed, with a tool a treating clinician could hold. Its success made the case that a focused, repeatable exam in the right hands changes outcomes. FAST opened the door the rest of point-of-care ultrasound walked through. Every later protocol, for the lung, the heart, the shock survey, followed the path FAST cut: a narrow question, a fixed sequence of views, an answer at the bedside in the minutes a decision allows. A clinician who learns FAST learns the shape of all of them. Four windows, one question, an answer fast enough to matter, scanned at the trolley as the team works to save a life.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.