Intraperitoneal Fluid Assessment Using Handheld Ultrasound in Trauma
After blunt trauma, free fluid inside the abdomen is blood until something proves otherwise. The handheld scanner exists, in this moment, to find it, or to fail to find it, before a patient who is quietly bleeding becomes a patient who is visibly dying. Everything else about the exam is detail in service of that one judgement.
The fluid does not announce itself.
It seeps. A torn spleen or liver weeps blood into the spaces between organs. The blood settles where gravity sends it, in volumes trivial in the first ten minutes and lethal an hour on. The whole skill of this exam is reading a quiet, shifting, gravity-bound thing through a probe pressed to the skin.
What blood looks like, and the lie it can tell
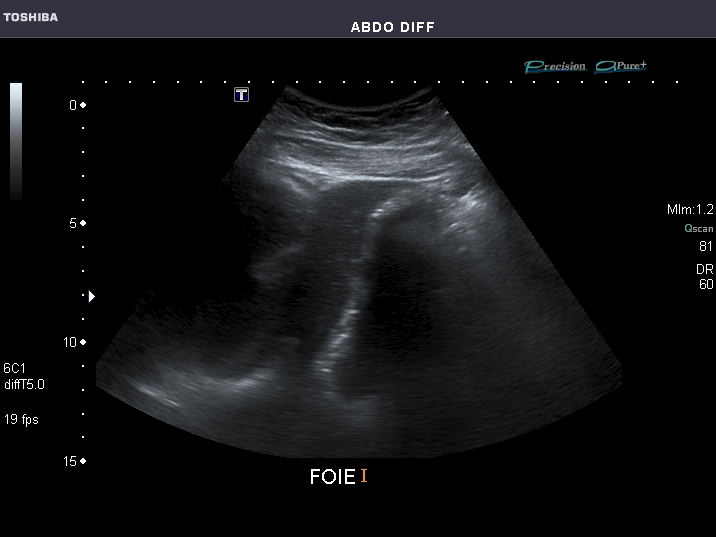
Free fluid reads black between organs; a fresh bleed shows clean and dark. (Ptrump16, CC BY-SA 4.0, via Wikimedia Commons)
Fresh blood is anechoic. It returns almost no echo. It paints the screen black: a clean dark wedge or stripe wherever it has pooled. This is the finding every trauma scan hunts, and in the first minutes it is usually honest: black means fluid, fluid means blood.
Then it begins to clot. The picture starts to lie. Clotting blood is not anechoic. As fibrin knits the red cells into a clot, the mass grows echoes of its own, turning grey, then almost tissue-coloured, until a fresh clot sitting against the liver can read as part of the liver. A clinician who learned that free blood is black, then stopped there, can sweep the probe across a clot and call the abdomen dry. The trap is real and it has cost lives. The defence is to know that the appearance of intraperitoneal blood is a function of time: anechoic when fresh, complex and echogenic as it organises, sometimes layered, with a dark serum supernatant floating over a settled cellular clot in a patient who has lain still. A clinician reading a trauma abdomen distrusts a too-perfect grey. They press to see whether a suspect area moves and deforms in the way a clot does and a solid organ does not. They weigh the picture against how long the patient has been bleeding. The black stripe is the easy positive. The grey clot, hiding in plain sight, is the one that separates a careful operator from a hurried one.
Black is fresh. Grey may be old blood, wearing the colour of the tissue beside it.
Where it goes
Gravity decides the map. In a patient on their back, three basins sit lowest: the recess between liver and right kidney, the space around the spleen, the pelvis behind the bladder. Blood from almost anywhere in the abdomen drains toward one of these. The right-sided recess catches the largest share, which is why it is scanned first and trusted above the rest.
Tilt the patient and the map redraws. A head-down tilt pulls fluid up toward the upper recesses; a head-up tilt sends it to the pelvis. A clinician with a stable patient and a faint suspicion can use this, tipping the bed to coax a small bleed into a window where it will be seen.
How little can be seen
The honest answer is: less than people hope, more than nothing. A skilled operator, scanning the right upper quadrant in a well-positioned patient, can detect somewhere around a couple of hundred millilitres of free fluid, sometimes less in ideal conditions, often more in a difficult body. The pelvis, with a full bladder as a window, can reveal smaller volumes still.
This number matters: it sets the floor of what a negative scan means. A clinic that treats any negative as proof of a dry belly forgets that a hundred millilitres of fresh blood, early, can hide below the threshold of even a good operator. The exam finds the bleed that has reached a detectable size. It is silent on the bleed that has not reached it yet, which is the entire reason a single scan is never the end of the story.
Scan it again
A bleed is a process, not a state. The scan that is empty on arrival can fill twenty minutes later as blood accumulates past the threshold. Repeating the exam, as the pressure drifts or the pulse climbs, turns a yes-or-no into a moving picture of a belly filling in real time.
Serial scanning is the quiet workhorse of this assessment. It costs no radiation, no contrast, no transfer. A clinician can run it as often as the patient’s course demands. A stripe absent at first and present on the third look declares a slow bleed that any single snapshot would have missed.
The fluid that is not blood
Not every black space in a traumatised abdomen is haemorrhage. A small amount of fluid in the pelvis is normal in many women. A patient with liver disease may carry ascites that predates the crash. A ruptured bladder spills urine; a torn bowel spills its contents. The exam shows fluid; it does not label the fluid’s origin.
Context names it.
A clinician reads a black space against the whole patient: the mechanism of injury, the vital signs, the volume and the speed of accumulation, the look of the fluid. A large, growing collection in a hypotensive crash victim is blood until the operating room proves otherwise. A trace of pelvic fluid in a stable young woman with a minor fall is, far more often, nothing at all. The same grey-and-black picture means different things in different bodies. The reader supplies the meaning the screen cannot.
Putting a number on it, roughly
Trauma rarely needs a precise volume. It needs a rough scale and a trend. A thin stripe in one window, in a stable patient, is watched. A deep pool spreading across several windows, in a patient whose pressure is sliding, is a surgical emergency. The count of positive windows and the thickness of the largest collection give a crude gauge that is enough to act on.
Precision is a peacetime luxury. In the bay, the question is not how many millilitres, only whether this patient goes to theatre now or can wait for a fuller scan. A black pool that grows between two looks answers that without a single measurement.
The traps that catch the unwary
Several things mimic free fluid, and a clinician who does not know them will see bleeding that is not there. The fat around the kidney can throw a dark line that apes a stripe of blood. A fluid-filled stomach or bladder can pose as a peritoneal collection. A mirror artifact can paint a phantom of the liver above the diaphragm. Each of these has a tell, learned with hours at the probe.
The mirror image of these false positives is the false negative, the deadlier of the two. A clotted bleed reading as tissue, a small early bleed below the threshold, a window obscured by gas or by a dressing: each lets a real bleed pass unseen. The discipline that protects the patient is the same on both sides. Read the picture against the patient, never alone. Distrust a finding that does not fit the story. Distrust a clean scan in a patient whose body says otherwise.
Finding the stripe
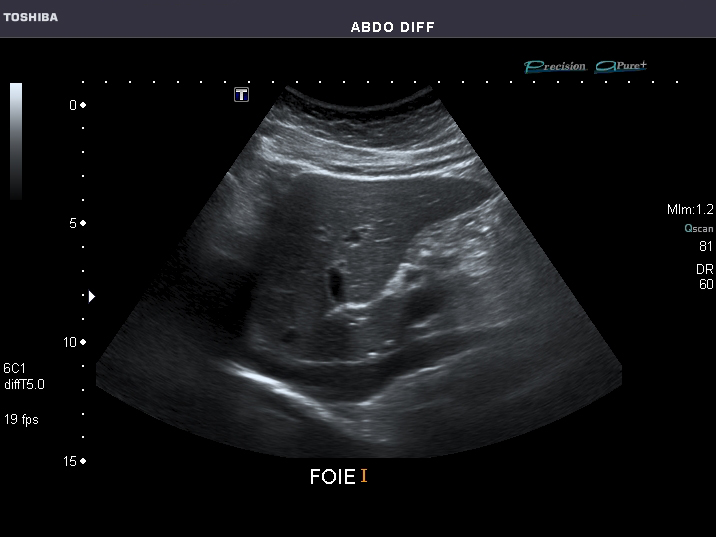
The positive is often a thin dark line, found by fanning slowly through the interface. (Ptrump16, CC BY-SA 4.0, via Wikimedia Commons)
The positive is often a sliver. Rarely a pool or an obvious black lake. More often a fine dark line tracing the edge between two organs, a few millimetres of anechoic fluid where pressed surfaces should meet with no gap at all. The eye has to be hunting for it to see it.
In the right upper quadrant the line to watch runs between the liver and the kidney. The likeliest spot is the lower tip of the liver, where the recess opens toward the pelvis and gravity delivers its first drops. A clinician fans the probe slowly through the whole interface, never freezing on one plane, since a thin stripe can sit in a slice a static image skips. The same care applies at the spleen, where the fluid more often gathers above the organ, against the diaphragm, than in the splenorenal line itself. In the pelvis the search runs behind the bladder and beside it, where even small volumes settle in a patient lying flat. Depth and gain need a moment of adjustment too. A fluid stripe set too shallow vanishes off the top of the screen. A gain pushed too high fills a true black space with false speckle that hides it. The technique is unglamorous and it is the bulk of the battle. A bleed that exists is found or missed less on the cleverness of the device than on whether the operator fanned through the right interface, at the right depth, with a hand patient enough to let a thin dark line declare itself.
What the evidence shows
The numbers from decades of study carry a clear shape. A focused look for free fluid is highly specific. When it shows a convincing black collection in a trauma patient, that fluid is almost always real and almost always matters. Its sensitivity is the softer figure. A meaningful share of patients with intra-abdominal injury show no free fluid on an early scan: the bleed is small, slow, or tucked behind the lining where the windows do not reach.
This asymmetry shapes how the result is used.
A positive scan is a strong reason to act, trusted enough to send an unstable patient toward surgery without further imaging. A negative scan is weaker evidence: a reason to keep watching, never a reason to relax. The clinician who takes this to heart reads a black pool as near-proof and a clean screen as a question still open. That single habit, treating the positive and the negative as findings of unequal weight, is what separates an assessment that helps from one that lulls a team into a dangerous calm over a bleed it has simply not seen yet.
The bleed the windows cannot reach
Some blood hides where the probe was never going to find it. The space behind the abdominal lining, the retroperitoneum, holds the kidneys, the back of the pancreas, the great vessels. A bleed there can be torrential and leave the front of the belly bone dry on ultrasound, since the blood pools behind the curtain the windows look in front of.
This blind spot is not a flaw to fix. It is a limit to respect.
A patient with a shattered pelvis can lose litres into the retroperitoneum with a clean trauma scan throughout. A team that reads that clean scan as reassurance reads it wrong. The mechanism of injury is the warning the ultrasound cannot give. A high-energy crash, a fractured pelvis, a stab to the flank: each raises the chance of a bleed in a place the probe does not see. The wise reader holds two thoughts at once. The scan is excellent at the question it can answer, silent on a whole compartment it cannot. A clean abdomen in a patient whose injury points to the back of it is a reason to reach for the imaging that sees what ultrasound cannot, never a reason to stand down.
What a positive changes
A confirmed pool of free fluid in a bleeding trauma patient is one of the fastest routes to a decision that ultrasound offers. There is no wait for a porter, a scanner, a report. The clinician who finds it acts on it: blood products, a call to surgery, a patient moved toward the theatre as the slower workup is still being booked.
That speed is the whole reason the assessment earns its place on the trauma trolley. The probe does not replace the careful imaging that follows in a patient who can wait for it. For the patient who cannot, it answers the only question that matters in the first minutes, with a tool already in the clinician’s hand, and the answer it gives can be the difference between blood replaced in time and blood lost past saving.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.