A multipurpose handheld ultrasound does the work of a whole shelf of probes from one base in a pocket. It carries a deep abdominal probe, a shallow vascular one, and a cardiac view, each swapped or shifted to fit the exam in front of it. One base and a handful of heads cover the bulk of what a clinic needs to scan.
What makes an ultrasound multipurpose
What a probe can see comes down to its sound. Low-frequency sound travels deep into the body and brings back a broad picture, so the convex probe runs there, reaching the liver, the kidney, a fetus, the aorta against the spine. The linear probe holds to the first few centimetres and draws fine detail in that shallow band, the thyroid, a vein, a tendon under the skin. A phased probe sends a narrow beam between the ribs to reach the heart in its cage of bone. Each head is a separate tool for a separate depth. No single one of them covers the whole body alone. The multipurpose device is the plain answer to that fact.
A device earns the word multipurpose when it carries that whole range. Some do it with a set of heads that snap onto one base, a convex for the belly, a linear for the surface, a phased one for the heart. Others build a single broadband probe that shifts its frequency across a wide span, working shallow and deep from one face. The base behind them does the same job either way. It drives the crystals, turns the echoes into a picture, and passes that picture to a screen. What changes from one exam to the next is the head in the hand and the depth it reaches.
The single-probe route trades a little quality for the convenience of never swapping anything. A broadband head that tries to be linear and convex at once is rarely as sharp at the surface as a dedicated linear one, nor as clean at depth as a true convex. The swap route keeps each head at its best, asking only a change of probe between exams. Nearly every multipurpose system picks one of these two paths. The choice runs through the whole feel of the device. The two roads simply feel different in the hand.
One base, the heads that snap on
The commonest multipurpose design splits the machine in two. The processing, the battery, and the link to the phone sit in a base. The probe is a separate head that plugs into it. To change the exam, the operator unplugs one head and snaps on another: a morning of abdominal scans runs on the convex head; an afternoon of vascular access runs on the linear one; a call to the resuscitation room takes the phased head for the heart. Only the head changes between exams. A good base senses which one is on and loads its settings before the gel is even down. This keeps the costly part, the processing and the screen, as one shared investment. The join is where the engineering is hardest. It has to carry dozens of electrical channels and keep them apart, hold the head square to a fraction of a millimetre, seal against the wipe-down a probe takes between patients, and survive thousands of swaps across the device’s life. A worn or dirty contact shows up as a flicker in the picture, so the connector is wiped and checked as part of the daily routine.
The economics drive the whole idea. A clinic buys the expensive base once and adds a head when a new kind of work arrives, with no second machine to buy. A practice that starts with abdominal scans can take on vascular access later for the price of a linear head. The base, the screen, and the software stay the same. A worn head is replaced on its own, at the price of a probe, the base untouched. A practice grows its imaging one transducer at a time.
The swap costs a few seconds and a moment of discipline. A head left on the wrong exam draws a poor picture, so the operator learns to match the probe to the depth before the scan begins. The device often names the head it senses and loads the preset to suit it. A good system makes the change quick enough that the choice of probe feels like part of the scan.
Some devices fold the whole range into one head, with no swapping at all. A single probe with a wide frequency band, switched in software, saves the swap, giving up the last edge of sharpness at each end. The trade is real on both sides. A clinic picks the path that fits how it works, weighing the make-up of a swap-head set against the ease of one probe that never comes off. Either way, the operator ends up with the right head for the depth in front of them.
The probes a multipurpose set carries
The convex probe is the workhorse of the deep body. Its curved face fans a wide wedge of low-frequency sound through the abdominal wall and across the pelvis, reaching the liver, the kidneys, the bladder, the aorta, and a pregnancy through the mother’s belly. The bulk of multipurpose work that goes deep runs on this head. It doubles as the general abdominal head and the obstetric one. Those two exams are the commonest reasons a clinic owns a scanner.
The linear probe is the tool for the surface. A flat face and a high frequency draw a crisp, square picture of the first few centimetres, the thyroid in the neck, a vein before a needle, a lump under the skin, a tendon or a muscle. It is also the head a clinician reaches for to guide a line into a vessel under direct view, the needle and the wall held in the same picture.
The phased probe is the small one for tight windows. Its little footprint slips between the ribs. Its beam opens into a wide sector beyond, the shape a cardiac scan needs to see the whole heart from a single narrow gap. Some sets add an endocavity probe for the close internal views of early pregnancy and the pelvis. Between three or four heads, one base reaches almost everywhere a clinical question lives.
Beyond the gray picture
A vascular scan in progress: color Doppler painting the moving blood on the screen, the probe held in the clinician’s hand. The same probe and the same color picture now come in a multipurpose handheld that fits a pocket. Image: Goleisureintl, CC BY 4.0.
The gray anatomy picture is only the start of what a multipurpose device reads. Two more modes ride on the same probe. Color Doppler lays a wash of color over the gray to show blood in motion, which way it runs and how fast: the flow that tells a live vessel from a still duct, the jet of a leaking valve, the empty space where a clot has stopped it. The operator switches it on with one button and reads flow without changing the head, the same probe doing two jobs at once.
M-mode trades the picture for timing. It takes a single line through the body and draws how the structures along it move, second by second, down the screen. It catches the slide of the lung against the chest wall, the beat of a fetal heart too fast to count by eye, the travel of a heart wall through one cycle. M-mode reads the rhythm a single frozen frame would let slip, motion drawn out as a line across time.
On-screen calipers turn each of these pictures into numbers, a length, an area, a volume, a velocity, measured off the frozen image and written into the report. A bladder volume comes from three diameters, a vessel’s narrowing from a pair of walls, a heart’s output from a sweep of one wall through a beat. The figures go into the report beside the pictures themselves.
Presets pull the modes and the settings together for each exam. One sets the depth, the gain, and the frame rate for a fast heart. Another settles them for a still, deep organ at the bottom of the screen. A third holds the low power a pregnancy is scanned at. The device loads the right preset when it senses the head and the kind of work, so the operator starts near a usable picture and tunes it from there.
Point-of-care, where it earns its place
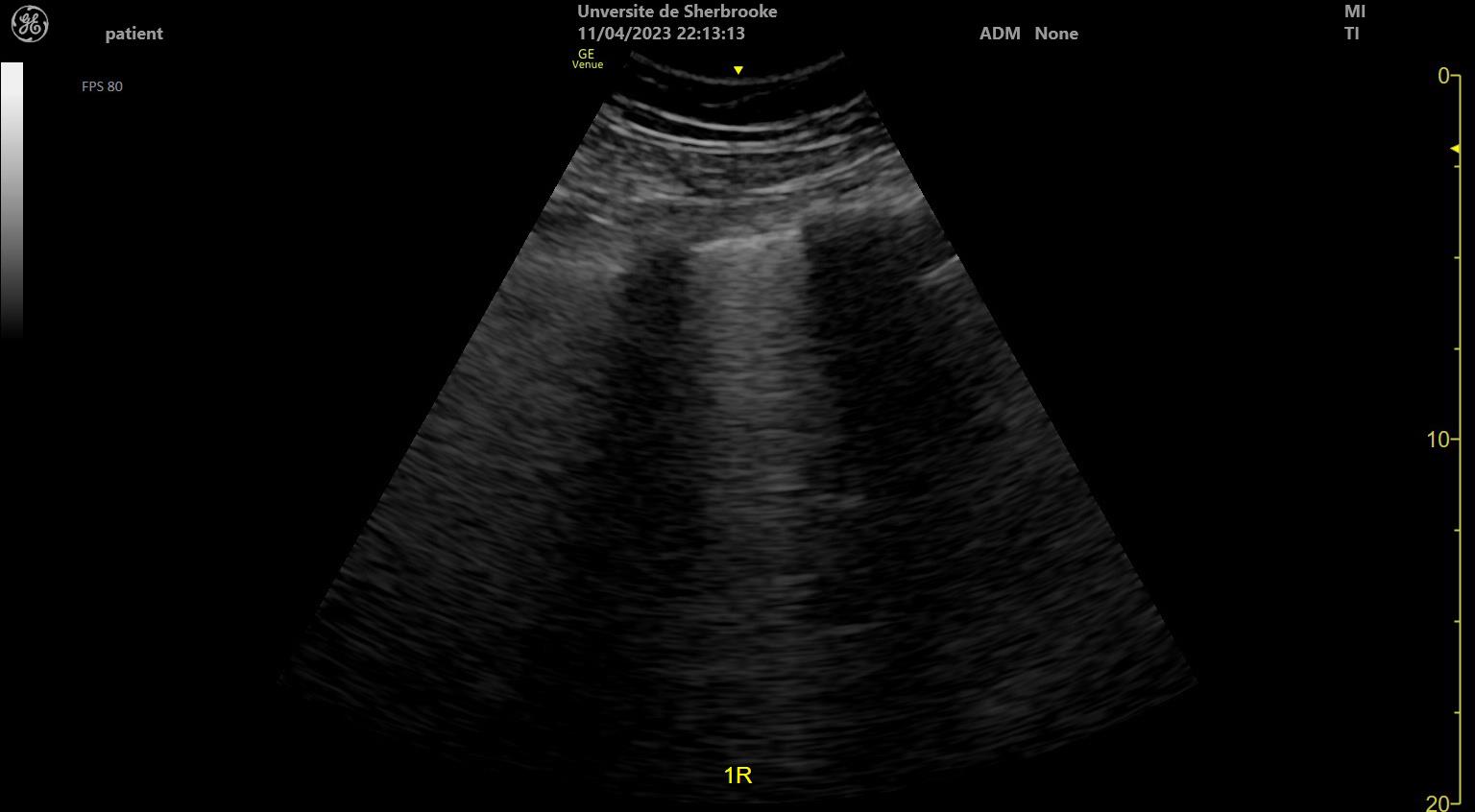
Lung ultrasound at the bedside. The bright beams fanning down from the top, the B-lines, mark fluid or scarring in the lung, one of the fast point-of-care reads a handheld is reached for. The “GE Venue” label, the depth scale down the right, and the MI and TI figures are the machine’s own readouts. Image: Tinss, CC BY-SA 4.0.
Point-of-care ultrasound is where the multipurpose device does its plainest work. A clinician carries it to the patient and answers one question on the spot, with a decision hanging on the answer. Is there blood in the belly after a crash. Is the lung sliding, or has it dropped. Is the bladder full, the vein open, the line sitting where it should. Each answer turns the next step at the bedside, with no wait for a department and no trip for the patient. The answer is on the screen before the trolley has stopped moving.
The strength of point-of-care work is speed. Its discipline is the narrow question. A focused scan asks one thing and reads it fast: free fluid yes or no, a heartbeat present or absent, a vessel open or clotted. It does not try to be the full hour-long study a sonographer runs with a cart. Reading too much into a quick look is the common trap, the answer stretched past what a focused scan can carry.
The focused exams an emergency clinician runs keep growing year on year. A trauma scan sweeps the belly and the chest for free fluid in a few windows. A lung scan reads the slide of the pleura and the lines that mark fluid in the air spaces. The same probe guides a needle into a deep vein, checks a bladder before a catheter, looks for a clot behind the knee, places a drain, confirms a tube, hunts a gallstone before a colicky belly is sent on. Each is a sharp question with a yes or a no at the end, the probe watching the needle the whole way in when a procedure needs a guide.
Emergency and critical care lean on this hardest. A patient too sick to move gets the scan at the trolley, in the resuscitation room, on the ward round. The device travels in a coat pocket and runs from a phone, so the picture comes to the patient in the place the patient already lies. For a team working against the clock, that speed is the whole value of the tool.
Reading the heart
The heart is the hardest of the common point-of-care targets. It lies behind the ribs and the lung, where sound is stopped, so it is reached through narrow windows between the bones and below them. The phased probe handles it. Its small face fits in the gap between two ribs. Its beam sweeps a wide fan from that tight starting point. From a single narrow slot between two bones, the whole chamber comes into view.
The bedside scan of the heart reads a few large things, the loud questions a crashing patient turns on. Does the heart squeeze well or weakly. Is there fluid in the sac around it, pressing the chambers. Is the right side swollen, the sign of a clot lodged in the lung. Is the big vein into the heart full or flat, a clue to the pressure inside and to how much fluid the patient can still take. These answers change the treatment of a crashing patient in the first minutes. They often decide whether the patient goes to the laboratory, to the operating room, or stays put for another look.
The rules a probe must meet
A probe that touches patients lives under a thick book of rules. Before a device reaches a clinic, it has to prove it is safe to the body it scans and that the picture it gives can be trusted. The rules cover the electricity inside it, the heat and pressure of the sound it makes, the cleaning it survives, and the claims its maker is allowed to print.
Two kinds of rule run side by side. One is safety. The sound a probe pours into tissue carries energy, measured as a heating index and a mechanical one. The standards hold both below the line where they could harm. The screen shows these numbers so the operator can keep them low. The other kind is proof. A maker who says a device measures a vessel or dates a pregnancy has to show the figure is accurate before the claim is allowed to stand. The list of tests is long and specific. Electrical safety, so no current leaks to the patient. A sealed body, rated for the fluid of a clinical day. The strength to take a drop onto a hard floor. A surface that holds up to repeated disinfection. The software itself, the part that turns echoes into numbers, is now judged as a medical device in its own right. A cleared probe has passed all of it, tested by someone other than the seller. The mark it carries is what lets a pocket scanner be trusted with the questions a hospital machine answers. A recall or a safety notice travels the same approved channels, so a probe already in use can be traced and pulled if a fault turns up.
Why wireless and handheld
The wireless form is what carries all of this into a pocket. The processing now sits in the probe and the phone it talks to, no bigger than a hand, with a radio link in place of a cable and a battery in place of a wall socket. The same phone stores the scan, attaches it to the patient, and sends it on to the next clinician. A quick look becomes a record someone else can open. A device this small goes where the patient is, on a ward, in a clinic, down a rural road, on a battlefield, which is the whole reason the multipurpose probe has reached into far more hands, and far more places, than the cart on its wheels ever could.
The phone does more than show the picture. It stores every scan against the patient’s record, labels and measures on the screen, and sends a study across a network to a colleague in seconds. A scan taken in a village reaches a specialist in a city for a second opinion. The smaller the device grows, the lower its price falls, so a single doctor can now afford a scanner of real clinical use. Deep imaging and shallow imaging, for them, have become affordable for the first time, deep work and shallow both within a single budget.
Who reaches for one
The multipurpose probe spreads widest where a full department is far away. An emergency physician keeps one in a coat pocket for the crashing patient. An intensive-care team reads a heart and a lung at the bedside without moving a ventilated patient an inch. An anaesthetist finds a nerve or a vein before a block or a line. Each of them reaches for the same device and asks it a different question of its own, reading the same kind of picture each time. The one probe rides from the trauma bay to the clinic room to the ward without a second thought.
Away from the hospital, it opens ground that had no imaging at all. A rural clinic dates a pregnancy and checks a swollen kidney where the nearest cart is a day of travel off. A midwife carries one in her bag on a home visit. A paramedic scans at the roadside, a ship’s medic far out at sea, a doctor in a camp running on a generator. The picture no longer needs the building it once lived in, only a charged battery and a pair of trained hands.
The thread through all of them is one. One person, one pocket device, one question that needs its answer now.
What a single device gives up
One device for everything has a cost. It shows at the edges. A probe that covers a wide range is rarely the sharpest at any single point in it. The deepest organ in the largest patient is the one place a high-end cart still does better. Breadth is paid for with a little quality everywhere, a price that rarely touches the focused question a handheld is reached for.
The demanding exams show the gap clearest. A full cardiac study, with its fine measurements of flow and wall motion, runs best on the processing of a large machine. A detailed obstetric anomaly scan calls for resolution at depth that only a high-end system holds. These exhaustive studies stay the work of a high-end cart and a specialist, run in a quiet room with the time and the depth of resolution they call for.
Upkeep asks its share too. A sealed probe wipes down between patients. A battery has to hold its charge through a full clinic round. A device that travels light is a device that has to take a knock and keep working. The connector that accepts the heads wears with every swap. It is built to a rated number of cycles before it is due for service.
Knowing the edge is the skill that makes the tool safe. A clinician who reads a clean handheld scan as a clean body, then stops, has trusted a quick look past its reach. The device catches the loud trouble in front of it. The multipurpose probe is a powerful first answer for the clinician who knows that edge and works inside it.
None of this is a fault in the design. It is the plain shape of a tool meant to do many jobs from one hand. A clinic that buys it for the wide reach and the bedside speed gets exactly what it pays for. Expecting a cart in a pocket measures it against the wrong machine.
The hand behind the probe
The last limit is the operator. A handheld picture is only as honest as the hand that holds the probe and the eye that reads it. A vessel missed by a poor angle, a heart read off a bad window, a shadow taken for a finding it is not: the device cannot catch these for the user. It cannot turn a novice into a reader. This is why point-of-care work leans so hard on the training behind the probe, and why the best devices spend as much effort on teaching the scan as on taking it.
One device, many jobs
One base, a few heads, and a phone: the multipurpose probe is the better part of an imaging department carried in a coat pocket.
Common questions about multipurpose handheld probes
What is a multipurpose ultrasound probe?
A probe, or a device, that covers several kinds of exam from one tool. It reaches the deep abdomen, the shallow vessels, and the heart by carrying different probe heads, or one broadband probe that shifts its frequency. The base behind them, run from a phone, drives all of it.
Can one handheld device do abdominal, vascular, and cardiac scans?
For everyday focused work, yes. A convex head reads the belly, a linear head the vessels, a phased head the heart, all on one base, each focused bedside question within reach of the pocket device. A full diagnostic workup is a different job, run on a high-end machine by a specialist.
What is point-of-care ultrasound?
Ultrasound done by the treating clinician at the patient’s side, to answer one question fast. It checks for free fluid after trauma, a sliding lung, a full bladder, a vein for a line. The scan is quick, a tool for a decision in the moment, apart from the long study a sonographer performs.
Does a handheld probe meet medical safety standards?
A cleared one does. Before sale, a handheld ultrasound is tested for electrical safety, for the heat and pressure of its sound, for the seal that lets it be cleaned, and for the accuracy of any measurement it claims. The IEC, FDA, and EU MDR marks are the proof it passed.
What can a multipurpose handheld not do?
The exhaustive study and the finest detail. A full echo lab, a detailed anomaly scan, a deep organ in a large patient: these reach past what a pocket device holds. They stay the work of a high-end machine. The multipurpose probe gives a first, fast, wide answer and leaves the last word to the full study.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.