RUSH Rapid Ultrasound for Shock and Hypotension Protocol
The patient is grey, cold, and dropping. The monitor shows a pressure that should not be that low, and the cause is anyone’s guess. This is the moment RUSH was built for. It is not the patient with an obvious bleed or a known heart. It is the one whose body has slipped into shock for a reason no history, no examination, no first round of bloods has named.
Guesswork is the old answer here. It is also dangerous. Pour fluid into a heart that is already failing and the lungs drown. Withhold it from a tank that is empty and the patient arrests. The treatments for the different shocks are not merely different; several of them are opposites; a wrong guess does active harm. RUSH replaces the guess with a look.
It takes minutes. The probe is already in the clinician’s pocket.
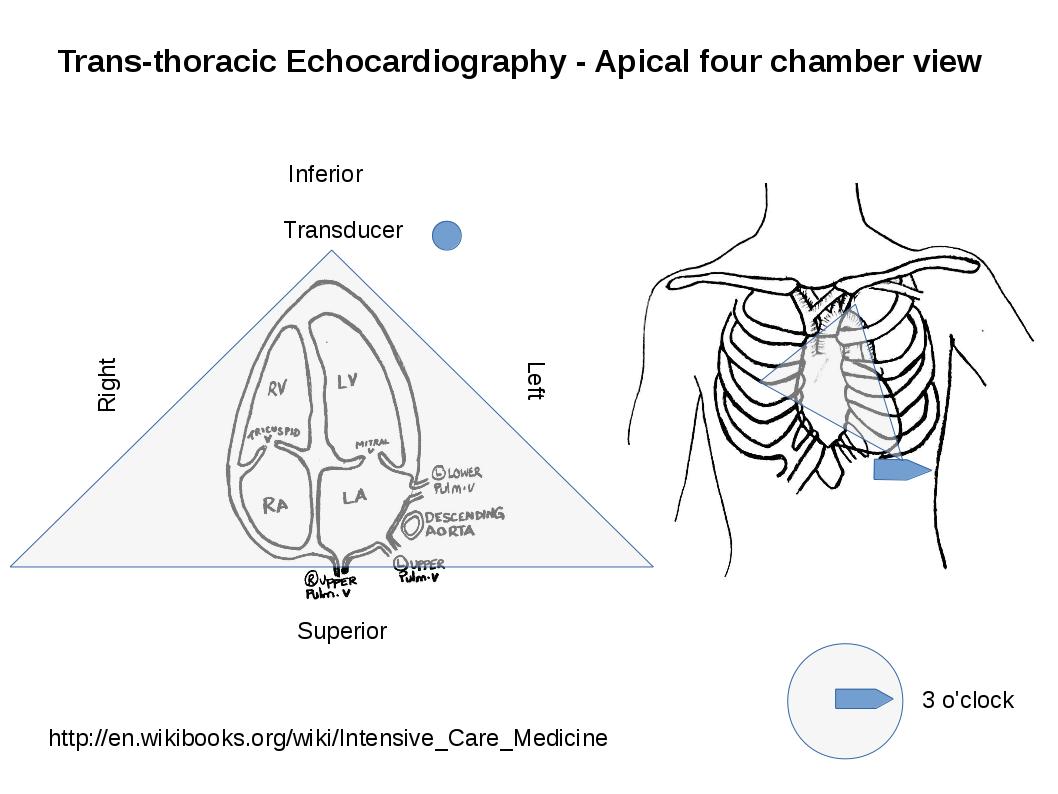
The pump: a focused cardiac view, read for squeeze, the sac, and the right side. (Balaji.md au, CC BY-SA 4.0, via Wikimedia Commons)
A plumber’s map of the circulation
The exam hangs on a metaphor a tired clinician can hold at three in the morning. The circulation is plumbing. There is a pump, the heart. There is a tank, the blood and the vessels that hold it. There are pipes, the great arteries and veins. Pressure falls when one of the three fails, . Each failure leaves a different mark the probe can read. The model is crude on purpose. Its whole value is that it survives panic. A clinician who cannot recall a textbook list of shock causes under pressure can still hold three nouns, and three nouns are enough to walk the probe across the body in order and let the images do the sorting.
Four shocks, four signatures
Underneath the metaphor sits the physiology that makes the whole exam work, and it repays sitting with, since every image RUSH reads is a window onto one of four ways a circulation fails. A pump that has weakened, in cardiogenic shock, cannot push its volume forward; the heart on the screen barely squeezes, the large vein behind it swells with blood that has nowhere to go, the lungs begin to flood as pressure backs up into them. An empty tank, in hypovolemic shock, shows the mirror image: a heart squeezing furiously and almost obliterating its own chamber with each beat, trying to make a pressure out of a volume that is not there. The great vein collapses flat with every breath. When the cause is bleeding, a black stripe of free fluid pools in the spaces the trauma windows watch. An obstruction, in obstructive shock, blocks the circulation at a single choke point: fluid in the sac throttling the heart from outside, or a clot in the lung swelling the right ventricle as it strains against a sudden wall of resistance. Dilated pipes, the shock of sepsis, leave a heart that often squeezes well and a tank that reads empty not for want of blood, only that the vessels have relaxed; the same volume now rattles around a larger space. Four mechanisms, four distinct pictures. The heart of the protocol is that a single sweep of the probe tells them apart at the bedside, in the window where the first drug or the first drain still has time to work.
That paragraph is the whole exam in miniature. The rest is just where to put the probe to read each sign.
Reading the pump
The heart comes first, scanned first for a reason: it answers more of the question than any other view. A clinician looks for three things. They read them at a glance, no measurement needed. Is it squeezing? A heart that flutters weakly points inward, at the pump itself. A heart that clenches down hard points outward, at an empty tank or open pipes. Is there a black rim around it, fluid in the sac building toward a tamponade that will close it off? Is the right side swollen out of proportion to the left, the bulge of a ventricle straining against a clot wedged in the lung? Three questions, one window. A clinician who reads them well has crossed nearly all the wrong answers off the list before moving the probe an inch.
Reading the tank
Two readings tell the tank’s story. The first is the great vein that returns blood to the heart, watched as it rises and falls with the breath. Full and still, it speaks of a circulation backed up. Thin and collapsing, it speaks of a patient who is dry. The second reading borrows the trauma windows, the flanks and the pelvis and the chest, hunting the black of fluid where the tank has sprung a leak.
A flat vein and a black belly, together, name a bleeding patient before a single drop has been sent for testing.
Reading the pipes
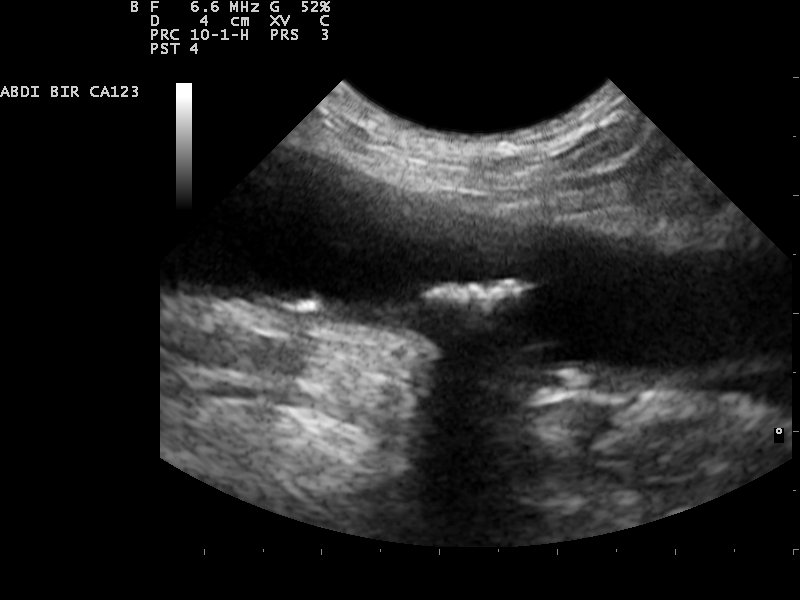
The pipes get two quick questions of their own. The abdominal aorta is measured across in a few seconds; a vessel ballooned beyond its normal calibre is an aneurysm, and a leaking one is a cause of shock the clock is already counting down. Then the large veins of the legs are pressed under the probe. A vein that refuses to flatten holds a clot. A clot in the leg is the likely parent of the one the swollen right heart hinted at upstream. The same clot can announce itself three times, in three places. The clinician who saw the strained right ventricle goes hunting its source in the leg with a fair idea of what waits there.
The tank gauge: the great vein, full or flat with the breath. (Nevit Dilmen (talk), CC BY-SA 3.0, via Wikimedia Commons)
The patterns the sweep reveals
No single image diagnoses shock. The sequence does. A barely-moving heart over a full vein is the cardiogenic pattern. A hammering heart over a flat vein, with or without a bleed, is the hypovolemic one. Fluid throttling the heart, or a strained right side with a leg clot, is obstructive. A vigorous heart over an empty-feeling tank, with no blood anywhere, points at the dilated pipes of sepsis.
Each pattern turns the resuscitation a different way. Several of those ways exclude each other: the fluid that saves the empty tank can sink the failing pump. The clinician who reads the pattern right starts the move that helps instead of the one that harms.
The vein that misleads
The great vein is the reading abused more than any other in the exam. A flat one usually means dry, a full one usually means backed up. The word usually is doing heavy lifting there. A ventilator inverts the breathing signs the vein gives. A young, athletic heart can hold a vein flat with volume to spare. A stiff old vein barely moves whatever the pressure. The vein is honest as a trend and treacherous as a single number. Watched as it fills under a cautious fluid challenge, it confirms a dry tank in a way one frozen frame never can. Trusted alone, in the wrong body, it sends a clinician confidently down the wrong road. The skill is to weigh it beside the pump and the leaks, never to crown it.
What the probe adds that the monitor cannot
A monitor reports a number. The blood pressure is low: the screen says as much in red. It says nothing more. The number names the emergency. It does not name the cause. A clinician staring at a falling pressure knows the patient is in trouble. They are no closer to knowing why.
A number is not a cause.
The probe answers the why. It does not improve on the monitor’s number; it explains it. A pressure of seventy means one thing in a heart that has stopped squeezing. It means the opposite in a heart hammering against an empty tank. The two patients need treatments that would each kill the other. The monitor cannot tell them apart. The probe can, in the time it takes to set it on the chest. This is the real shift RUSH brought. It is not a finer measurement of how sick the patient is. It is the first quick window onto what is making them sick, read from the body itself instead of guessed from the figure on the wall.
A film, not a photo
One sweep is a snapshot. Shock moves. The picture that fits the patient on arrival can be wrong twenty minutes later, once a litre of fluid or a worsening bleed has redrawn it.
The pipes: the abdominal aorta, measured across in seconds. (Nevit Dilmen, CC BY-SA 3.0, via Wikimedia Commons)
The exam earns its keep on repetition.
A clinician runs it, treats, then runs it again to read the answer the treatment wrote. A flat vein that plumps up after fluid confirms the tank was dry and the fluid was right. A pump that stays weak as the pressure climbs warns that the fluid is filling lungs instead of vessels. The repeat scan turns RUSH from a single guess at the cause into a running commentary on whether the resuscitation is working. It costs nothing to repeat: no dye, no radiation, no trip down a corridor. A clinician reads the patient as a film instead of a photograph, correcting course before there is no course left to correct.
Where the exam runs out of road
RUSH sorts the common shocks fast. It is weakest where shock hides best: when more than one cause runs at once. A septic patient can also carry a tired heart. A bleeding patient can also throw a clot. The exam tends to show the loudest cause and fall quiet on the second, and a clinician who stops at the first answer can miss the one still killing the patient underneath it.
The reading never stands alone. It sits beside the history, the trend of the numbers, the response to the first treatment. A pattern is a powerful clue and never a verdict. Used as the opening sort of an undifferentiated shock, weighed against everything else the patient is saying, it is among the best uses a probe has. Asked to be the final word, it overreaches, the way every focused exam does when pushed past the question it was built to answer.
A worked read
Picture the grey patient again. The probe goes to the chest first. The heart is barely twitching, the walls sluggish, the chambers wide. That alone reshapes the next move. This is no tank to flood.
The probe slides to the flank. The great vein is fat and motionless, no give with the breath, the picture of a circulation dammed behind a failing pump. The flanks are dry, the pelvis dry, no leak anywhere. A glance at the front of the chest catches the first vertical beams of fluid creeping into the lungs.
The read is complete in under two minutes: cardiogenic shock. The treatment writes itself. Support the pump, hold the fluid a guess would have poured in, hunt for why the heart failed. Run the same probe over the hammering heart and the flat, collapsing vein of a different patient. The answer flips to an empty tank and the fluid the first patient could never have taken. Two grey patients, two low pressures, two opposite treatments, told apart by a probe in the minutes that decide which of them lives.
What it changed
Before the probe, a clinician facing this patient reasoned in the dark and treated by trial, watching the monitor to learn whether the last move helped or hurt. RUSH put a light on the cause. The same handheld carried for the trauma survey runs it. The tool is already at hand when the grey patient rolls in. The deeper gift is the structure more than the pictures. Pump, tank, pipes is simple enough to survive the worst minutes of a shift. It lets a clinician under real pressure recall the whole exam and read it fast. It turned the department’s hardest patient from a guess into a sequence of plain questions with visible answers. A clinician who learns it stops gambling on the cause of shock and starts seeing it. That single shift is why the protocol travelled into emergency and critical-care medicine the world over.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.