Abdominal Aortic Aneurysm AAA Emergency Screening With Handheld Probe
An older patient arrives with pain in the back or the belly and a pressure that is quietly sliding. The pain reads like a kidney stone, like a pulled muscle, like a dozen harmless things that fill a shift. Underneath the ordinary story, the main artery of the body may be splitting open. A ruptured abdominal aortic aneurysm kills fast and kills quietly, wearing the mask of lesser troubles until the patient collapses on the trolley. The probe asks one plain question in under a minute, the question the history keeps hiding. Is the aorta too wide.
A wide aorta in this patient is an emergency.
The classic picture, a pulsing mass with pain and a falling pressure, arrives complete only late, and often not at all in the heavy belly where no mass can be felt through the wall. The examining hand misses what the probe shows at a glance: the plain calibre of the vessel itself, the one fact that decides everything.
What a wide aorta means
The abdominal aorta runs down the back of the belly, a thick muscular tube carrying the body’s whole output toward the legs. A healthy one measures around two centimetres across, holding that width from the chest to the navel. When its wall weakens, it balloons outward under the constant pounding of the pressure inside. A vessel grown to three centimetres or wider is an aneurysm, a bulge in a pipe that never rests. The bulge widens slowly across years, the wall thinning as it stretches, the danger building in silence until one day the wall gives. A tear empties the circulation into the belly faster than a team can answer.
Width is the measure of the danger, and the numbers are blunt. A three-centimetre aneurysm is watched. A five-centimetre one is referred for repair before it bursts. Past five, the risk of a tear climbs with every added millimetre, steeply enough that size alone can force the decision to operate. Below five centimetres the watching is itself the treatment, a scan repeated over the months and years to catch the slow widening early. The single number on the screen, the plain diameter of the vessel, carries the whole weight of what happens next.
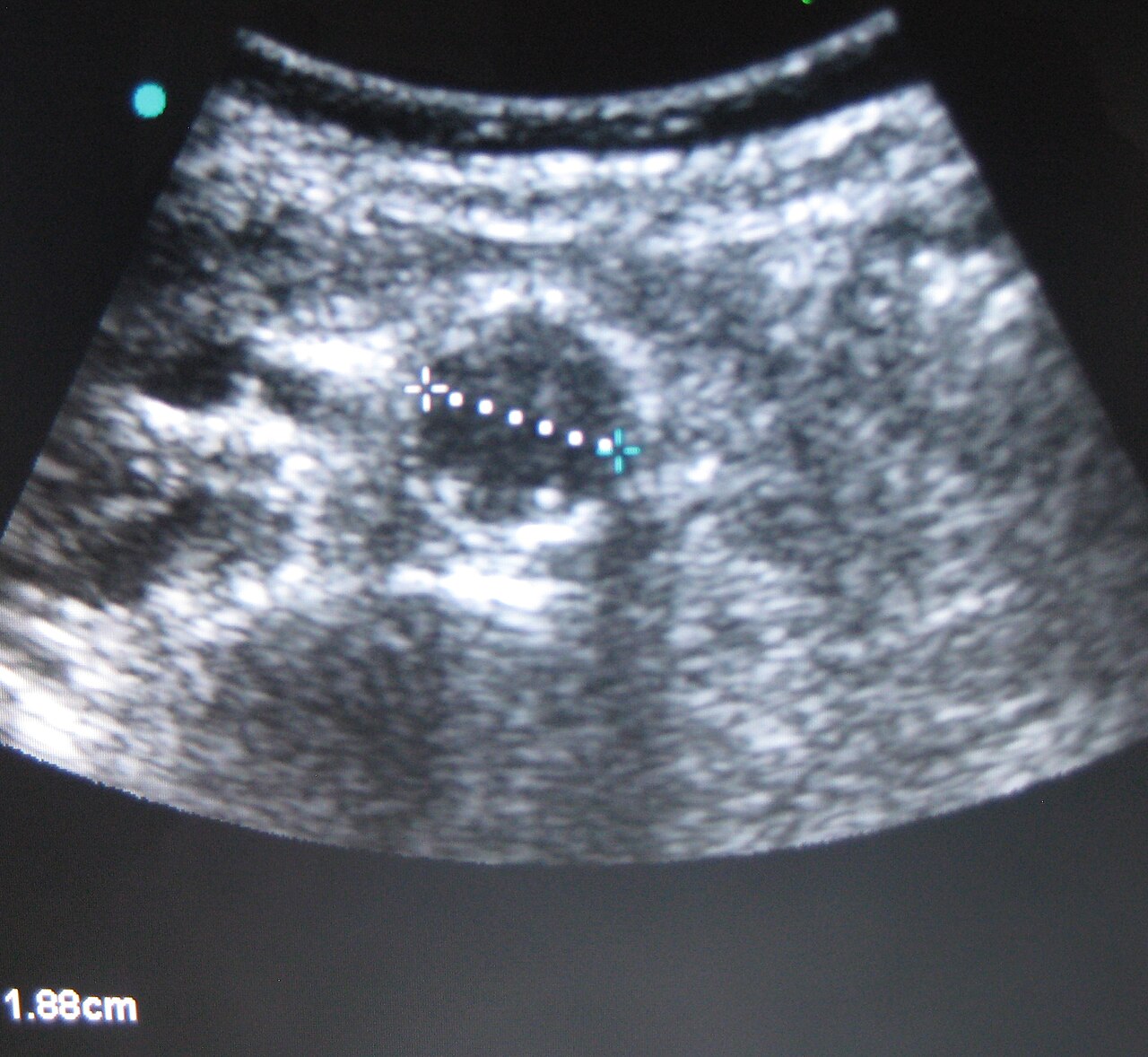
A normal abdominal aorta on ultrasound, measured in cross-section. Wikimedia Commons, CC BY-SA 3.0
Finding the vessel
The scan opens in the upper belly with a curved probe held across the body. The landmark is the spine, a bright curved line throwing a dark shadow into the deep of the image. The aorta sits just in front of it and a little to the patient’s left, a round, thick-walled circle that pulses hard with each beat of the heart. The clinician sets the probe below the breastbone, finds the spine first, then finds the pulsing circle resting against the front of it, and knows at once which vessel is which.
From there the probe slides down the belly, following the aorta toward the navel and below. The vessel narrows a little as it descends, then splits into the two arteries that carry blood into the legs. The clinician tracks it the whole way, since an aneurysm can hide low, near the split, where a single look high in the belly would sail straight past it.
Follow it from the ribs to the split.
The one measurement
Everything in the exam comes down to a single measured number. Measuring it well is the difference between a reading that saves a life and one that quietly misleads. The diameter is taken in short axis, the probe held square across the vessel, the shape on the screen a true cross-section, a real circle in place of a smear. An oblique cut, the probe tilted off square, slices the tube at a slant and draws an oval wider than the vessel truly is, manufacturing an aneurysm where none exists. The clinician squares the probe until the lumen is round, then measures across the widest part of it. The calipers run from the outer edge of the wall on one side to the outer edge on the other, outer to outer, never lumen to lumen. The reason is a quiet one with teeth. An aneurysm often packs itself with layered clot along its inner wall, a thrombus that hugs the lining and narrows the channel the blood still flows through. A clinician who measures only that open channel reads a near-normal width and walks away from a large aneurysm stuffed with clot. The true size is the whole vessel, wall to wall, the clot counted in. The threshold then sorts the patient with a few plain cuts: under three centimetres is a normal aorta, three to five is an aneurysm kept under watch, beyond five is a vessel heading for repair. The physics under those numbers is a law of tension. The stress pulling a vessel wall apart rises with its radius. A wider aorta carries a higher wall tension at the same blood pressure. The tension climbs faster as the vessel grows, a small gain in width bringing a large jump in the force working to tear the wall. That steep climb is why a five-centimetre aneurysm is a different animal from a four, and why the number is measured with such care. A single reading is never the whole story. The aneurysm can be focal, a saccular out-pouching on one short stretch of an otherwise ordinary tube. The clinician measures along the entire length, never at one spot alone, since a normal segment says nothing about the one sitting above or below it.
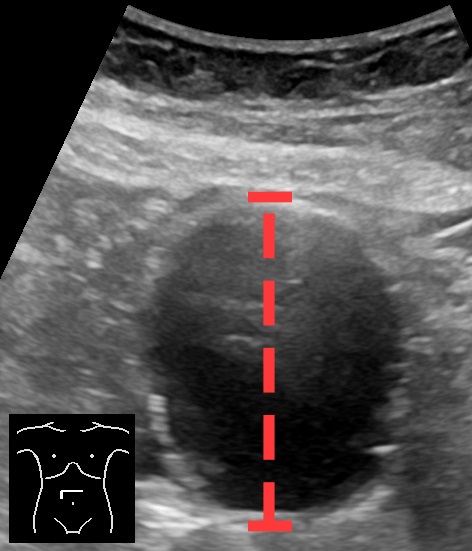
An abdominal aortic aneurysm in axial view, measured outer wall to outer wall. Wikimedia Commons, CC0
Aorta or vena cava
The vessel beside the aorta fools a new eye. The vena cava, the great vein returning blood from the legs, runs alongside the aorta to the patient’s right. The two look alike at a careless glance, a pair of dark circles deep in the belly. Their differences stand out once they are known. The aorta is round, thick-walled, pulsing hard with the heart, holding its shape against any pressure from the probe. The vena cava is oval, thin-walled, shifting its shape with the breath, flattening readily under a gentle push of the hand.
Mistaking one for the other sends the whole reading wrong. A clinician who measures the vena cava and calls it the aorta can miss an aneurysm beside it, or invent one where none exists. The cure is to name the vessel by its wall, its pulse, its place against the spine before a single caliper is set.
What the probe cannot see
The exam finds the aneurysm well. It sees the rupture itself poorly, and that gap is the gravest thing to grasp about it. When an aneurysm tears, the blood escapes into the space behind the lining of the belly, the retroperitoneum, a compartment the standard windows do not reach. The probe shows a wide aorta with great confidence. It rarely shows the blood leaking out behind that aorta. A clinician who waits to see the rupture before acting waits for a picture the probe was never built to give, and waits as the patient bleeds.
The reading is read with the patient, never alone. A wide aorta in someone with pain and a falling pressure is a ruptured aneurysm until an operation proves otherwise, whether the leak is seen or not. The diameter and the patient together make the call. A clean-looking retroperitoneum on the screen offers no reassurance, since it is the one place a fatal bleed loves to hide.
The enemy is gas
Gas in the bowel is the great obstacle to the view. Air scatters the sound before it reaches the aorta, blanking the deep belly with a grey haze that hides the vessel entirely. The defence is steady, patient pressure with the probe, pressing the gas-filled bowel aside to open a clean window to the vessel behind it. A patient who can bend their knees relaxes the belly wall and helps the cause. Rolling the body onto one side lets the heavy bowel fall away from the vessel, opening a path the upright belly kept shut. Time and a gentle, persistent hand win nearly every view a first glance seems to deny.
Against the CT scanner
The scanner down the corridor is the fuller test by far. A CT shows the aneurysm, the rupture, the exact shape and reach of both, the detailed map a surgeon needs to plan the repair. The probe shows far less. It answers one question, the diameter, at the bedside in a minute, with a tool already in the clinician’s hand. The trade is speed against detail. A stable patient with time to spare goes to the scanner for the full picture. The corridor, the lift, the wait for a free slot: each is a stretch of minutes a leaking aorta does not grant. An unstable one, crashing in the bay, cannot survive the trip down the corridor, and the probe decides the next move where the patient lies.
The unstable patient cannot travel. The probe goes to them.
The symptomatic patient decides it
The number means one thing in a well patient and another in a sick one. A four-centimetre aorta found by chance in a comfortable patient is a referral, a thing to watch and to repair in good time. The same four centimetres in a patient pale and hypotensive with belly pain is an alarm that cannot wait, since even a smaller aneurysm can leak under the right strain. The diameter sets the suspicion. The patient sets the urgency. The two are read together, never apart.
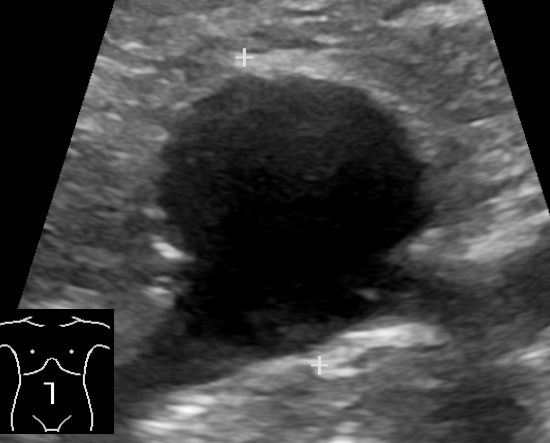
A saccular abdominal aortic aneurysm in sagittal view. Wikimedia Commons, CC0
The traps
Several errors catch the hurried operator. The oblique cut that fattens a normal aorta into a false aneurysm is the commonest, cured by squaring the probe until the lumen reads truly round. A calcified wall throws a bright shadow that swallows the far edge, tempting a short measurement that undersizes the vessel. The vena cava posing as the aorta misleads the entire exam from its first frame. A measurement of the open channel alone, the clot ignored, undersizes a vessel that is already dangerous.
Each trap shares one root: a reading taken too fast. The defence is a square cut, an outer-to-outer caliper, the whole length scanned, the vessel named against its neighbours. The discipline costs a minute and protects the answer that a minute saved would have spoiled.
Learning it
The exam is among the quicker scans to learn to a useful level. Finding the round, pulsing aorta against the spine takes an afternoon of trying. Measuring it square and outer-to-outer takes a little teaching and a little practice at the probe. The sign itself is bold: a circle either under or over three centimetres, read in seconds once the vessel is found and squared. The harder lessons are the traps, the oblique cut and the hidden clot and the vena cava in disguise, the errors a learner comes to know best by meeting them under a teacher’s eye.
Finding the aorta is easy. Measuring it honestly takes care.
What it changed
Before the probe, a ruptured aneurysm was a diagnosis made on a table, or guessed at as a patient was rushed toward a scanner they did not live to reach. The clinician facing belly pain and a low pressure reasoned from the odds and lost the gamble too often, sending a leaking aorta home as a kidney stone or a strained back. Ultrasound put the aorta on a screen in the resuscitation bay, answering in a minute the question whose delay had cost the lives.
The gift is a fast, plain answer to a deadly question. The probe does not replace the scanner that maps the repair. For the patient who cannot reach that scanner, the probe finds the wide aorta that explains the crash, turning a fatal guess into a measured decision made at the bedside in time to act on it. That single shift, from a guess to a number, is why the screening probe has earned its place on the resuscitation trolley beside the trauma tools.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.