Pleural Sliding Sign Detection With Handheld Ultrasound
Lay a probe on the front of a chest and watch the bright line where the chest wall meets the lung. If that line shimmers with each breath, a fine glitter sliding back and forth, the two layers of pleura are touching and moving over each other as they should. That shimmer is lung sliding, the single best thing a probe can find on a chest in a hurry. Its presence, at the spot under the probe, all but rules out a pneumothorax there. Its absence raises the alarm. A whole branch of emergency ultrasound rests on reading this one small flicker right.
The shimmer is the sign.
Lung sliding is read in seconds and learned in minutes. The eye finds the pleural line, settles on it. It asks one plain question: does it move. A flickering line is a lung pressed to the wall and breathing; a still line is a warning that wants chasing down.
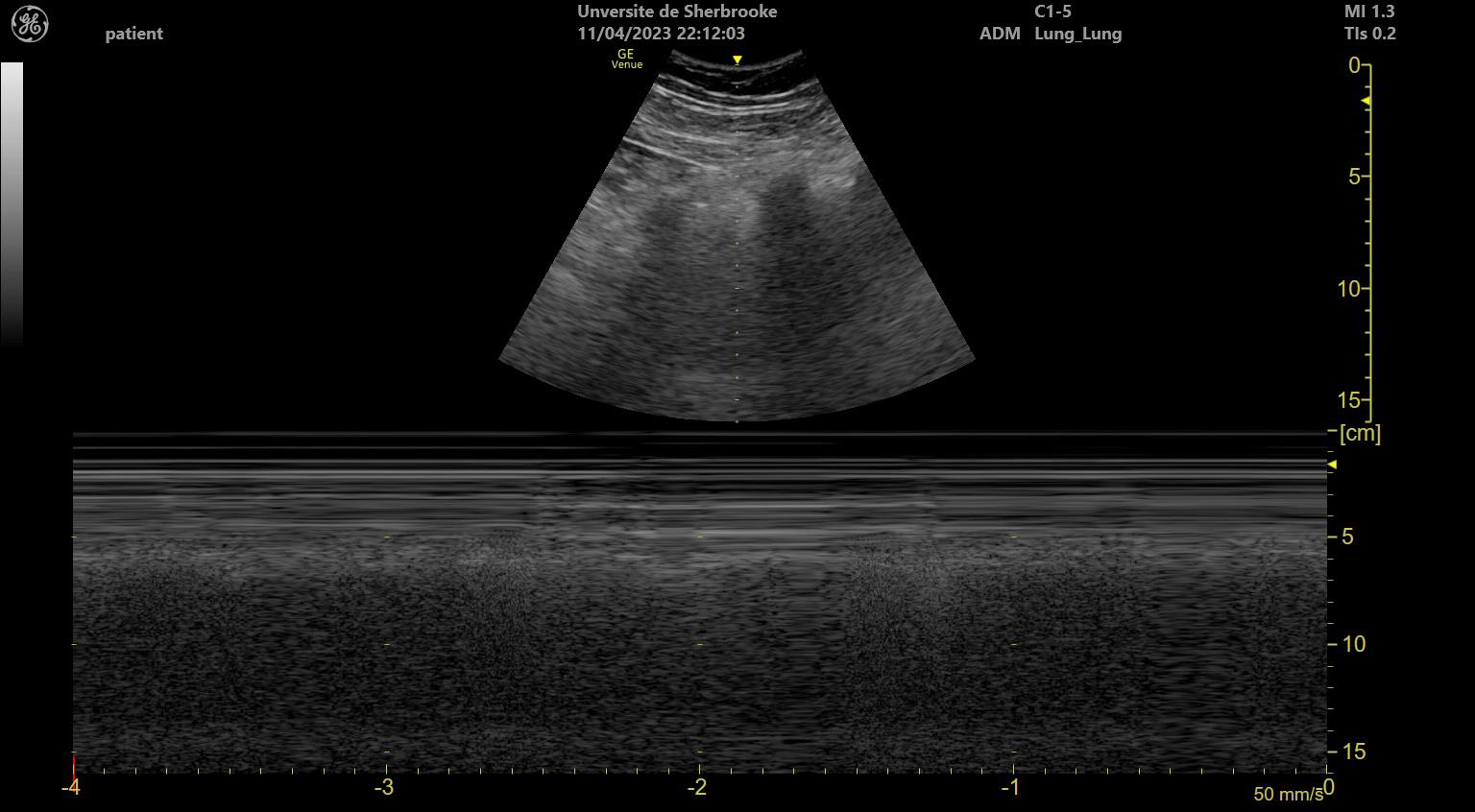
The seashore sign in M-mode: calm lines of the chest wall above, granular sand of the sliding lung below. Sliding present rules out a pneumothorax at that spot. Wikimedia Commons, CC BY-SA 4.0.
What the shimmer is
Two thin membranes line the space between lung and chest wall. The parietal pleura clings to the inside of the ribs; the visceral pleura wraps the lung itself. In health the two lie pressed together, a film of fluid between them. The lung glides under the ribs with every breath. Ultrasound catches that glide as a twinkling, shimmering motion right at the pleural line, the two layers sliding one across the other. The motion is small, a millimetre or two at the surface; a high-frequency probe held still over one rib space reads it best, its fine detail catching a glide a deeper probe would blur. A calm hand matters more than a powerful machine; the shimmer shows itself to an eye that waits a breath or two for it.
A pneumothorax breaks the contact. Air leaks into the space between the membranes and pushes the lung away from the wall. The visceral pleura, riding on the lung, drops out of reach of the probe. The parietal pleura left against the ribs does not move with the breath. The shimmer dies. A still pleural line, where a breathing lung should glitter, is the first hint that air has crept in where it should not be. Free air, lighter than the lung, rises to whatever part of the chest sits highest; in a patient on their back it pools at the front, the first place the probe should look and the place the shimmer is soonest lost.
Sliding present: the lung is touching the wall. Sliding gone: something has parted them.
Seashore and barcode
The eye can be fooled by a faint shimmer, which is why the probe offers a second, harder reading through M-mode, a setting that trades the moving picture for a single line of it drawn out over time. Pick one scan line through the pleura and the machine plots what sits along it moment by moment, stacking those moments left to right into a strip that turns motion into a still pattern a clinician can study without trusting a flicker. Above the pleural line lies the chest wall, which does not move, so M-mode draws it as a stack of flat, calm, horizontal lines, a set of parallel stripes running straight across the strip. Below the pleural line lies the sliding lung, and that constant shimmer scatters the beam into a grainy, sandy, stippled texture with no straight lines at all. The result is a picture with a sharp divide: still horizontal stripes on top, granular sand below, split by the bright pleural line between them. Clinicians call it the seashore sign, the calm sea of the still chest wall meeting the sandy beach of the moving lung. It is the mark of a lung that slides. Take away the sliding, as a pneumothorax does, and the grainy sand below the pleura vanishes, since nothing down there moves any more. The horizontal stripes of the motionless chest wall now run straight through the pleural line and onward to the bottom of the strip, top to bottom, an unbroken field of parallel lines with no beach at all. This is the barcode sign, named for its likeness to the stripes on a label, or the stratosphere sign, for the high flat calm it shows. A seashore says the lung is sliding and the pleura touch; a barcode says the sliding is gone and air may have parted them. The two patterns are blunt, quick to tell apart. They put a frozen record of the motion on the screen that the eye alone could miss in a faint or a frightened chest.
Seashore, the lung slides. Barcode, it does not.
Seashore versus barcode. The sand below the pleural line marks a sliding lung; when sliding stops, the stripes run straight to the bottom. Original illustration.
The lung point
One finding turns a suspicion into proof. A pneumothorax rarely fills the whole chest; the lung stays partly inflated and touches the wall over some region, falling away from it over the rest. Somewhere a border runs between the two. Place the probe at that border and the screen shows a lung that slides for part of the breath, then drops away to stillness as the collapsing edge passes under the beam. That alternation, sliding giving way to no sliding at the same spot with each breath, is the lung point. It is found nowhere but a pneumothorax.
The lung point seals the diagnosis. A flickering pleura rules a pneumothorax out; a lung point rules it in, the one place on the chest where the inflated lung and the pocket of air meet and trade places under the probe. The border drifts a little with each breath as the lung swells and shrinks; the probe is held steady over one spot until the flip shows itself, a patient look rewarded by the surest mark the chest can give. Sweeping the chest to find that border, then watching it flip from beach to barcode, gives a bedside certainty a plain film struggles to match. A supine film, taken through the whole depth of the chest, can flatten a front-lying pocket of air into the general grey of the lung behind it; the probe reads only the surface, where that same pocket lies plainest.
Find the point where sliding starts and stops: that is the edge of the air.
When stillness lies
A still pleural line is a sensitive sign, never a specific one. Lung sliding can vanish for reasons that have nothing to do with free air. A clinician who reads every barcode as a pneumothorax will chase shadows. A lung stuck to the wall by old scarring or a deliberate pleurodesis does not slide, the membranes fused where they should glide. A lung that is not being ventilated does not slide either, as when a breathing tube has slipped too far and feeds only one lung, leaving the other still under the probe.
Severe disease mutes the shimmer too. A lung stiff with dense consolidation or end-stage scarring barely moves, the sliding faint to absent over the worst of it. A patient holding their breath shows no sliding for those seconds, the lung simply not moving. Each of these can mimic the stillness of a pneumothorax to an eye that reads motion alone. The list is short and learnable, each entry a state where the lung sits quiet for a reason of its own, none of them free air in the space.
Absent sliding asks a question; it does not answer one.
The way past the trap is to gather more than the one sign. A lung point, if found, settles it. The lung pulse, read next, rescues many of the false alarms, separating a lung that sits still against the wall from one that has been pushed away from it.
The lung pulse
A motionless lung still feels the heart. The beating heart sends a faint tremor through the chest. A lung pressed against the wall picks it up, the pleural line giving a tiny rhythmic jump in time with each beat even when no breath moves it. The jump is small, easy to miss without a steady hand, clearest in M-mode where each beat prints a faint vertical tick against the still stripes of an unmoving chest. Clinicians call this the lung pulse, and its meaning is precise: if the pleura twitches with the heartbeat, the two membranes are touching, so no air sits between them: no pneumothorax sits under the probe.
The pulse rescues the still lung. A lung that is not ventilated, a held breath, a mainstem-intubated chest, all show no sliding yet keep the lung pressed to the wall. All keep the lung pulse beating through. A true pneumothorax has parted the membranes, so the heart’s tremor cannot cross the gap. The lung pulse dies along with the sliding. The pulse is read in the same window as the glide, one more glance at the same pleural line, costing the clinician no extra time at the bedside.
No sliding, but a pulse: the lung is touching. No sliding and no pulse: suspect the air.
Finding it, step by step
The exam runs a short, fixed course. Lay a high-frequency probe on the front of the chest, high, where free air gathers first in a patient lying flat. Find the pleural line between two rib shadows, the bright stripe that the ribs frame. Settle the eye on it and watch through a few breaths for the shimmer of sliding.
Confirm what the eye saw with M-mode. Drop the cursor through the pleura and read the strip: a seashore of sand beneath calm stripes means the lung slides; a barcode of stripes running top to bottom means it does not. The frozen pattern guards against a faint shimmer misread in a tense moment. A photograph of the strip, saved to the record, lets a second reader check the call later, a small proof that outlasts the live scan.
Read further when the line sits still. Look for the lung pulse, the heartbeat’s tremor crossing a touching pleura. Sweep the chest outward in search of a lung point, the border where sliding gives way to stillness. A pulse or a sliding zone nearby pulls the diagnosis back from pneumothorax; a clean lung point drives it home.
Read every spot against the patient and the rest of the scan. A barcode over a chest scarred by old disease means something other than it would over a healthy one. The history tells which. The sign is fast and strong, sharpest as one piece of a fuller look rather than a verdict read off a single still line. Used that way, inside its limits, the sliding sign is among the quickest certainties a crashing chest can give, a few seconds of watching that can turn a resuscitation in the right direction.
What it changed
Before the probe, a pneumothorax in a supine patient was easy to miss. Free air rises to the front of a chest lying flat, the place a supine film sees worst, so a dangerous pocket could hide on an X-ray until it grew large enough to threaten the circulation. The clinician listened, tapped, waited on the film. The clinician sometimes met the air only when the patient began to crash.
Lung sliding put the answer in the open. A shimmer found at the bedside clears the pleura under the probe in seconds. A still line with a barcode and a lung point names the air long before a film would. The sign reads the front of the chest, the spot the supine film fails, turning a diagnosis that once leaned on luck and time into one a probe settles on the first pass.
The deeper gift was a sign anyone could learn. Sliding is bold, quick, read after a handful of scans, and the M-mode strip backs the eye with a record. A finding that once waited on a chest film and a careful eye now flickers on the screen the moment the probe touches down, the same small glitter read alike in a trauma bay and a clinic far from any radiology suite.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.