Lung Ultrasound B Lines Assessment For Pulmonary Edema Diagnosis
A patient fights for breath, and the cause is the question the next drug depends on. Wet lungs, drowning in fluid backed up from a failing heart, need water pulled off and the heart eased. Dry lungs, an airway disease tightening down, need the opposite. Pour fluid off a dry chest and the patient suffers for nothing; treat a flooded chest as though it were dry and the patient drowns. The probe sorts the two in a minute, reading the water in the lung straight off the screen.
Bright vertical lines mean water below.
The reading hangs on a single artifact, a beam of brightness the lung throws when fluid creeps into it. Count those beams and a clinician reads how wet the lung has grown, before a chest film is shot, before the bloods return, with the breathlessness still carrying a cause that can be turned around. The answer arrives at the bedside, in the time it takes to lay a probe on the chest and watch a breath pass.
The question that splits the breathless
Breathlessness wears one face for a dozen causes. The heart that cannot clear its load and the lung that cannot move its air look alike across a room, both gasping, both frightened, both starved of air. The history blurs them, since many patients carry both a tired heart and a worn lung at once, and a long night offers little time to tease the two apart. The treatments pull in opposite directions. A clinician guessing wrong loses ground fast, and the patient pays for the delay.
The lung holds the answer in its water. A heart failing backward floods the lung tissue with fluid pressed out of its overloaded vessels. An airway disease leaves the lung dry behind its tightened pipes. The amount of water in the lung is the fork in the road, and the probe reads it directly off the screen.
What a B-line is
A B-line is an artifact, not a structure. Grasping that is the key to reading it. The probe cannot see into a healthy lung at all. Air reflects sound almost completely. A normal aerated lung returns only a set of flat horizontal echoes called A-lines, the plain reverberation of the pleural line repeating down the screen at even intervals. A dry lung is a lung of A-lines. The picture changes the moment fluid arrives. The lung is built of countless tiny air sacs, threaded by thin partitions, the interlobular septa, that carry its plumbing between them. When the pressure in a failing heart backs fluid into the lung, that fluid seeps first into these septa, swelling them as the air sacs around them stay full of air. The probe now meets a thing it cannot ignore: a tiny pocket of fluid hemmed in by air on every side. Sound striking that boundary bounces back and forth between the fluid and the air, trapped, ringing, sending a long train of echoes to the probe over and over. The machine paints that ringing as a single bright vertical beam shooting from the pleural line straight to the bottom of the screen. That beam is a B-line. Each fluid-filled septum under the probe throws its own beam. A little fluid throws a few scattered beams. More fluid swells more septa and throws more beams, until the beams crowd together and merge into a sheet of white, a lung flooded enough that the screen glows. The beams are a gauge of the air-to-water ratio of the lung, read without a single measurement taken. A clinician counts brightness and reads wetness. The genius of the sign is that it turns an invisible thing, fluid buried deep in lung tissue, into a bright artifact a beginner can spot, since the worse the flooding grows, the more the screen lights up to show it.
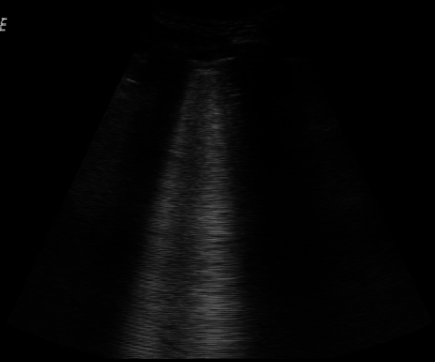
B-lines on lung ultrasound: bright vertical beams rising from the pleural line, the mark of a wet lung. Wikimedia Commons, public domain
Reading a true one
A bright vertical line is not always a B-line, and the difference matters, since the lung throws up several look-alikes that mean nothing at all. A true B-line answers to a short list of features, each one earned. It begins exactly at the pleural line, springing from that bright stripe and no deeper. It runs straight down the screen to the bottom, never fading partway.
It is sharp and bright, a clean laser of a line against the grey around it. It erases the horizontal A-lines wherever it passes, wiping them from its path. It moves side to side with the sliding of the lung, swinging as the patient breathes, never sitting fixed on the screen.
Pleural line to screen bottom, bright, erasing, moving.
The look-alikes fail one test or another. A short comet of brightness that fades before the bottom is something else. A vertical streak that does not spring from the pleural line, or one that sits still as the lung slides beneath it, is some other artifact wearing the same colour. The discipline is to demand every feature before counting a line as real.
Counting false lines floods a dry lung with imagined water. A clinician who sets the bar low, calling every streak a B-line, turns a healthy chest into a failing one on paper and treats a disease the patient does not have. The features are the guard against that error.
From a few to a white lung
The number of B-lines tracks the depth of the flooding. A normal lung shows none, or perhaps one or two at the base, where gravity gathers a little fluid in almost anyone. Three or more crowded into a single field of view mark that field as wet. As the heart fails harder, the lines multiply and thicken, drifting toward one another across the screen until the gaps between them close. A field with three or four scattered beams reads as mildly wet; a field where they have fused into a glowing sheet reads as a lung losing its air to water.
Merged beams are a lung half-drowned.
The pattern of a wet heart
Heart failure writes a signature in the way the B-lines fall. The flooding is even, spread across both lungs in a mirror image, since a backed-up heart loads the whole circulation alike. It favours the lowest parts, heaviest at the bases where gravity pulls the fluid down, easing toward the tops. The pleural line above the beams stays thin and smooth, the lung surface itself unharmed, only waterlogged behind it. Bilateral, gravity-bound, smooth-lined, symmetric: that pattern, in a breathless patient, points hard at a heart that has failed.
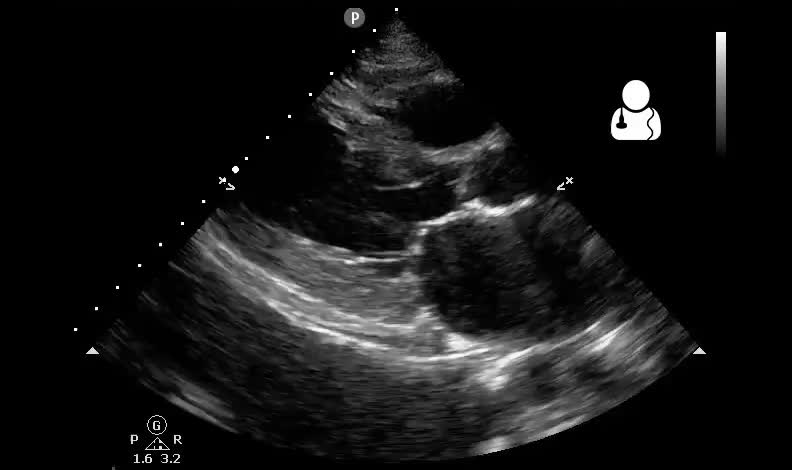
Bedside lung ultrasound in a hypoxic, breathless patient. Ultrasound of the Week / Wikimedia Commons, CC BY-SA 4.0
The pattern matters more than the count. A handful of B-lines spread evenly and low, in a patient short of breath, carries the heart’s signature even before the fields turn fully white. A clinician who reads the distribution reads the cause, never the number standing alone.
The pattern that is not the heart
Other floods leave other marks. Telling them apart is the harder half of the skill. A scarred, fibrotic lung throws B-lines too. Its pleural line is thick and ragged where the heart’s stays smooth, the lines sitting in a fixed, patchy spread that spares whole regions and holds unchanged across months. Pneumonia floods one zone and leaves the rest dry, a focal cluster of B-lines over an angry, broken pleural line, often with a patch of airless lung beneath it. The lung of severe inflammation shows the same patchiness, drowned areas sitting beside spared ones. A clinician who knows only that B-lines mean fluid sends a fibrotic lung toward the diuretics a failing heart would need, draining a patient who was never overloaded in the first place.
The distinction is read in the pleural line and the spread. Smooth line, even spread, both bases: the heart. Ragged line, patchy spread, spared zones: the lung itself. The same bright beams, read by the company they keep, point toward opposite diseases.
Counting across the chest
A single window is never enough on its own. The clinician scans a set route across both sides of the chest, upper and lower, front and flank, reading each field as wet or dry and building a map of the whole. A few fields wet low on both sides reads quite differently from every field drowned. Eight fields, four to a side, is a common sweep, quick to run and broad enough to catch the spread that names the pattern. A clinician who scans one or two spots alone can miss a patchy flooding, calling a wet lung dry by landing the probe on a spared field. The route is the safeguard: the same fields in the same order on every patient, ensuring a soaked corner is never quietly skipped.
Watching the fluid leave
The sign earns its keep twice over in the watching. B-lines are not a one-time yes or no. They rise as a lung floods and fade as it dries, tracking the water in the tissue in near real time. A clinician who treats a wet heart, pulling fluid off with a drug or a dialysis machine, can scan again an hour on and watch the beams thin out, the A-lines return, the lung dry before their eyes. The picture guides the dose in a way no single snapshot can. The diuretic or the dialysis is titrated against the lung itself, against a number that falls as the water leaves, in place of a blind guess at how much to give.
What B-lines are not
The beams are sensitive and unspecific, and respecting that keeps a clinician honest. They rise with any process that swells the lung’s interstitium with fluid or scar: heart failure, inflammation, infection, fibrosis, the lung injury of severe illness. A field of B-lines says the lung in that field is wet or scarred. It does not say why on its own. The why comes from the pattern, the pleural line, the patient in front of you, the way the picture moves over hours.
Lung ultrasound in a patient short of breath. Ultrasound of the Week / Wikimedia Commons, CC BY-SA 4.0
Bright beams name wetness, never its cause.
The traps
Several errors mislead the hurried eye. A gain turned too high paints false beams across a dry lung; a gain set too low erases the real ones. A probe held over a rib instead of a rib space throws shadows mistaken for lines. A few basal B-lines in an older patient can be a normal finding misread as failure. The cure is a clean technique and a refusal to read the count alone, weighing it always against the pleural line, the spread, and the whole of what the patient brings. Read with that care, the count becomes a measurement; read without it, a guess dressed up as a number.
Learning it
The sign is among the fastest in all of ultrasound to learn. A bright vertical beam erasing the horizontal lines is bold, caught in minutes, far easier to see than the subtle motion of a sliding lung. A learner counts B-lines well on the first day. The harder part comes later, in reading the pattern: telling the smooth even flooding of a heart from the ragged patchy flooding of a sick lung, the lesson that takes the cases and the months.
Counting beams is easy. Reading the pattern takes time.
What it changed
Before the probe, the wet lung and the dry one were told apart by a stethoscope’s crackle, a chest film read too slow, a blood test back in an hour. The clinician treated breathlessness half-blind, often starting both treatments at once and waiting to see which one helped. Ultrasound put the water in the lung on a screen in a minute, turning a guess at the cause into a reading taken at the bedside in time for the choice to matter.
The deeper change is a number that moves. The breathless patient is no longer a single hard guess; they are a picture that can be watched, scanned as the treatment works, the beams thinning as the lung dries. A clinician reads the cause, then reads the cure taking hold, all from the same bright lines climbing or falling on the screen.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.