Lung Ultrasound A Lines Normal Pleural Pattern Recognition
A breathless patient need not have a sick lung. The surest finding a chest scan can return is a normal one, a lung dry and aerated, breathing as it should. That finding is as useful as any disease, since it clears the lung off the list and turns the search elsewhere. The mark of a healthy lung surface is a pattern of plain horizontal lines, the A-lines, repeating down the screen below the pleural line. Reading them is reading a lung at rest.
A normal lung has its own signature.
The skill of spotting disease rests on knowing health first. A clinician who cannot recognise a normal lung at a glance cannot trust the moment one turns abnormal. The A-lines are that baseline, the quiet pattern every other finding is measured against. Learn the quiet pattern first; every loud one then stands out the sharper for it.
The value of a quiet lung
Finding a dry lung answers a loud question quietly. A patient gasping for breath could be drowning in a flooded lung or fighting a tightened airway, and the two need opposite care. A chest full of A-lines, the lung sliding beneath them, says the tissue is dry and aerated. The flood is ruled out at that spot. The search swings toward the airways, the clot in the lung, the causes that leave the lung surface itself looking well. A flooded lung and a dry one demand opposite first moves. The probe makes that call before a single drug is chosen, sparing the patient the harm of a treatment aimed at the wrong organ.
Recognising normal is half the exam. The clinician who reads only disease misses the power of a clean scan, the way a dry lung in a breathless patient redraws the whole list of what could be wrong. A confident normal is a finding in its own right. It carries real weight, narrowing a differential and changing a plan as firmly as any shadow or stripe a clinician hunts for.
What an A-line is
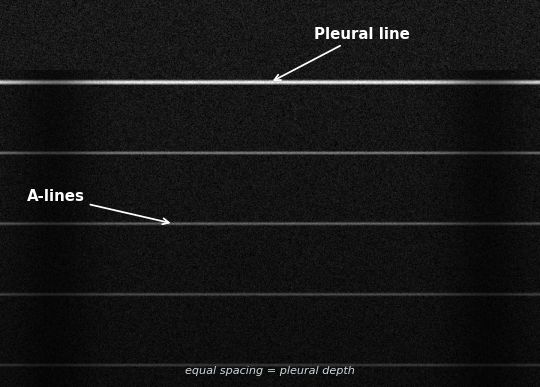
An A-line is an echo of an echo, not a thing in the lung. The pleural line, where the chest wall meets the lung, is a near-perfect mirror to ultrasound, since the air-filled lung behind it reflects almost all the sound that reaches it. A pulse of sound leaves the probe, strikes the pleural line, and bounces straight back. The machine draws the pleural line at the depth that first bounce implies. A portion of that returning sound, reaching the probe face, bounces back down, strikes the pleural line again, returns to the probe a second time. The machine, knowing only the time each echo took, draws this second, later echo as a fainter line at twice the depth of the pleura, mistaking the longer round trip for a deeper structure. The bounce repeats, drawing a third line at three times the depth, a fourth at four, each fainter than the one above it. The result is a ladder of horizontal lines below the pleural line, evenly spaced, the gap between them equal to the depth of the pleura itself. Those are A-lines. They are not tissue. They are the same pleural reflection printed again and again at multiplying depths, the screen’s way of saying that nothing save air lies beneath the pleura. That last point is the heart of the matter. A-lines appear whenever the space behind the pleura is full of air, reflecting the sound completely, whether that air sits inside a healthy breathing lung or inside the free space of a pneumothorax. The artifact reports total reflection at the pleural line. It cannot tell why the reflection is total. A clinician who reads A-lines as proof of a normal lung, with no further test, has read only half the picture, since the same ladder can stand over a collapsed lung with air trapped against the wall. The A-line says the sound met air and turned back. What that air is, the artifact leaves for the next sign to settle.
A-lines as a schematic: horizontal echoes repeating below the pleural line at equal spacing, the depth of the pleura set as the gap. Original illustration.
The normal profile
A-lines alone are half a finding. The other half is motion. A normal lung surface shows the A-lines and, at the pleural line above them, the shimmer of lung sliding, the two pleural layers gliding over each other with every breath. A-lines with sliding is the picture of a dry, aerated, healthy lung surface. Clinicians give it a name: the A-profile.
The A-profile is the lung’s all-clear for water. Where it shows, the tissue is dry: no fluid in the septa to throw B-lines, no flooding to glow white. In a breathless patient, an A-profile across both chests pushes hard against a diagnosis of heart failure, since a failing heart floods the lung and erases the A-lines under a rising tide of B-lines. A clean A-profile, found across the lower chest, stands among the strongest single arguments against an acute cardiac flood that a bedside scan can offer.
A-lines plus sliding: the lung is dry.
The reading is quick once the eye holds both halves at once. The horizontal ladder says dry. The shimmer says the lung is touching the wall and moving with the breath. Together they read normal in a second, a clean baseline a clinician can return to as a patient’s chest changes through a long night. Each repeat scan is read against that first clean picture, a drift toward B-lines flagged the moment the dry ladder starts to break.
The dangerous twin
The A-lines hide a trap that has cost lives. They appear over a pneumothorax exactly as they appear over a healthy lung, since trapped air reflects the sound just as completely as breathing air does. A clinician who sees the A-lines and calls the lung normal, without checking for the sliding, can miss a collapsing lung dressed in the pattern of health. The horizontal ladder looks reassuring. Standing over still, sliding-less pleura, it is a warning instead. The whole danger turns on a single habit: the eye that has learned to demand the sliding before trusting the ladder, every time, with no exception made for a chest that looks calm.
A-lines without sliding are a pneumothorax until proven otherwise.
Reading the dry lung in a breathless patient
The A-profile sends the search down a clear path in a patient short of breath. The lung is dry. The flood of heart failure grows unlikely. The breathlessness springs from somewhere the lung surface looks well: a tightened airway, a clot lodged in the lung, a process that spares the air sacs. The dry lung does not name the cause. It narrows the field sharply. From a list that began with the lung, the heart, the vessels and the airways all in play, the dry reading strikes the flooded lung from the running and hands the clinician a shorter, sharper set of suspects.
The next step looks at the legs. A dry-lunged, breathless patient with a clot in a leg vein carries a clot in the lung until proven otherwise, the dry chest and the leg clot together pointing at a pulmonary embolism. The lung surface looks well since the trouble sits in its vessels, never its air. The probe travels from chest to leg inside the same brief exam. Two windows, the chest and the leg, settle a diagnosis that once waited on a scan down the corridor a sinking patient might not have survived to reach.
The handheld probe that returns the A-line pattern at the chest wall. Wikimedia Commons, CC BY 4.0.
A dry lung sends the probe to the legs.
With no clot in the legs, the path turns to the airways. A dry lung, sliding well, no leg clot, in a patient wheezing and fighting for air, points toward an airway disease, the asthma or the chronic lung that tightens the pipes, the tissue itself left dry behind them. The A-profile has walked the clinician from a flooded differential down to a focused one. The same dry ladder that ruled out the flood now points, by what surrounds it, toward the airway as the likely seat of the trouble.
This is the quiet power of the normal pattern. A finding of nothing wrong with the lung surface is the hinge the whole diagnosis turns on, swinging the search from the lung to the heart, the vessels, the airways. The dry lung speaks by what it rules out. A negative finding, read with confidence, can move a diagnosis as far as any positive one ever does.
What A-lines do not promise
A normal lung surface is not a normal patient. The A-profile reads the surface of the lung, the first centimetre the sound reaches before the air turns it back. A clot deep in the lung’s vessels, a disease of the heart, a poisoning of the blood: none of these touches the pleural line, and all of them can kill a patient whose lung surface reads perfectly dry. The A-lines clear one organ’s surface. They say nothing of what lies deeper or elsewhere in the body. A confident A-profile is a reason to look harder elsewhere. It is no reason to stop. A clinician who treats it as an all-clear for the whole patient reads far more into the ladder than the ladder ever said.
A dry lung surface is reassurance, never a discharge.
The traps
A few errors turn the pattern false. A gain set high can blur the A-lines into a grey wash that hides them; a gain too low can fade them from view entirely. Other horizontal artifacts can ape an A-line for an untrained eye, lines that do not sit at the clean multiples of the pleural depth a true A-line keeps. The gravest error stays the old one: reading the A-lines without reading the sliding above them, and mistaking the pattern of a pneumothorax for the pattern of perfect health. Every one of these is undone by the same care: a clean gain, an eye trained on the true spacing of the ladder, the sliding always checked before the pattern is called normal.
Learning to see normal
The pattern is among the first things a learner should fix in the eye. A-lines are bold and regular, easy to recognise after a handful of scans. The harder discipline is the habit that must come with them: never to read A-lines alone, always to check the sliding above, always to ask what the dry lung means for the patient lying there. The pattern itself is simple. The reflex that must surround it takes building, scan after scan. The learner who sees the ladder in a day and learns to distrust it without the sliding over the weeks that follow has gained a pairing of habits the lung rewards across a whole career.
See the ladder, then check it slides.
What it changed
Before the probe, a normal lung was a thing of exclusion, reached only after the films were read and the bloods returned with nothing to show. The clinician treated a breathless patient down a long list, ruling the lung out slowly and last. The A-profile lets the lung be cleared in a minute, at the bedside, on the first pass, freeing the search to chase the cause the dry lung has quietly uncovered. What once took an hour of waiting now takes a breath of scanning. The time saved is time the real diagnosis is treated in. The lung stops being the slow last box to tick and becomes the first one cleared.
Recognising health turned out to be half the art. A clinician who knows the A-profile cold reads a normal lung as fast as a flooded one, and uses the normal to steer the search as surely as any abnormal sign. The quiet ladder of A-lines, read with the sliding above it, is the place lung ultrasound begins. A trainee meets it on the first day and leans on it for a whole career, the single pattern that turns up on nearly every chest a probe is ever laid against, the steady ground from which every stranger finding is judged.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.