Breast Ultrasound BI RADS Classification Handheld Imaging System
BI-RADS turns a vague impression of a breast finding into a number that carries a known cancer risk and a set next step. Where one reader might call a mass probably fine and another a bit worrying, the system fixes a category, from a clear normal scan up to a proven cancer, each tied to what to do next. On ultrasound the reader describes the mass by a fixed set of features, and those features decide the category. The letters stand for Breast Imaging Reporting and Data System, from the American College of Radiology.
What BI-RADS sets out to do
BI-RADS gives every reader the same words and the same scale. Before it, one report called a lump suspicious and another called it probably fine, with no shared meaning behind the words. BI-RADS fixes a lexicon of features and ties the final category to a written action. A category 2 sends the patient back to routine screening. A category 4 sends her to biopsy. The number is the part the referring doctor acts on.
The system runs across mammography, ultrasound and MRI, with the same seven categories on each. The category is the bottom line of the report. The features behind it explain how the reader got there. A reader who writes a category without the features has skipped the work that backs it.
Ultrasound has a place in breast imaging for two jobs that a mammogram cannot do. It sorts a mass into solid or cystic, which settles many findings on the spot. It also reads the dense breast, where overlapping tissue hides a cancer on the mammogram. A handheld probe does both at the bedside, with no booking and no radiation.
BI-RADS does more than guide one patient. It supports an audit. A center tracks how many of its category 4 masses turn out to be cancer, and the rate shows whether the readers call the category well. The fifth edition, current since 2013, sharpened the ultrasound lexicon and tightened the wording behind each category, so two readers reach the same words for the same mass.
The seven categories
BI-RADS runs from 0 to 6. Each number carries a meaning and a next step, so the category is a plan as much as a label.
Category 0 is incomplete. The scan needs another view or another test before a call can be made. Category 1 is negative, a normal breast with nothing to report. Category 2 is benign, a finding with no cancer risk, such as a simple cyst or a calcified fibroadenoma. Both 1 and 2 return the patient to routine screening on the usual schedule.
Category 3 is probably benign. The finding looks benign, with a cancer risk under 2 percent. It goes to a short-interval follow-up, usually at six months. A biopsy is held back unless the finding grows or changes. A stable result over two years moves it down to benign.
Category 4 is suspicious, and it splits three ways to grade the worry. Category 4a carries a 2 to 10 percent chance of cancer. Category 4b carries 10 to 50 percent. Category 4c carries 50 to 95 percent. All of category 4 goes to biopsy. The split tells the patient and the doctor how much weight the result will carry as they wait for it.
Category 5 is highly suggestive of cancer, above 95 percent. It goes to biopsy with surgery already in view. Category 6 is a cancer already proven by biopsy, used on follow-up scans as the patient moves through treatment.
The category sets the schedule as much as the call. A category 1 or 2 waits a full year for the next routine scan. A category 3 comes back in six months, then again, until two years of stability move it down to benign. A category 4 or 5 moves within days to a needle. The number tells the patient the risk and the pace of what comes next.
The five ultrasound features
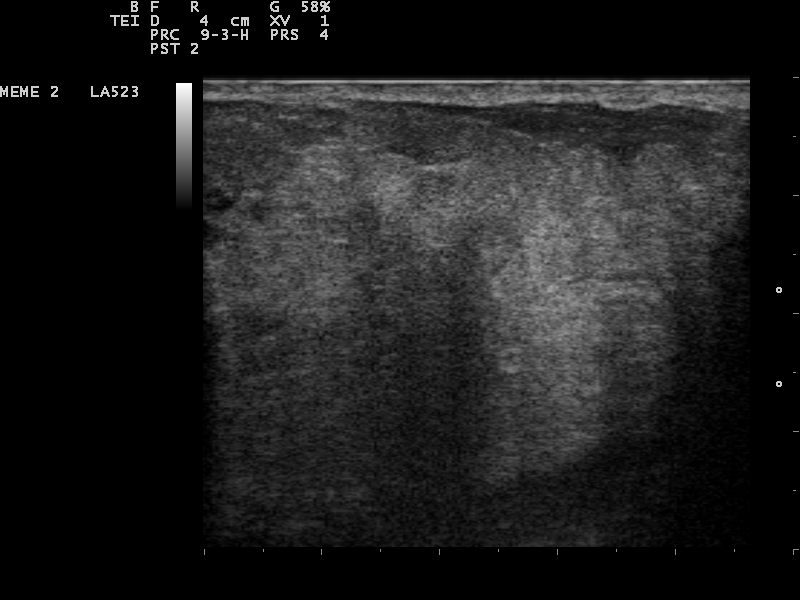
A hypoechoic area in the breast. The reader scores its shape, orientation, margin, echo pattern and posterior features to reach a BI-RADS category. Image: Nevit Dilmen, CC BY-SA 3.0, Wikimedia Commons.
The category does not come from a guess. It comes from five features the reader scores on every mass. Shape is the first. A mass is oval, round, or irregular. An oval mass is usually benign. An irregular one raises concern. Orientation is the second. It is the feature unique to ultrasound. A mass that lies parallel to the skin, wider than it is tall, is usually benign. A mass that stands taller than it is wide, across the tissue planes, is a worry for cancer. Margin is the third. A circumscribed margin, clean and sharp all the way around, fits a benign mass. A spiculated margin, with sharp lines radiating out, is a strong sign of cancer. Microlobulated and ill-defined margins sit between the two. Echo pattern is the fourth. A mass can be anechoic, the black of a simple cyst, or hypoechoic, the darker grey of a typical solid mass. A complex mass holds both fluid and solid parts. Posterior features are the fifth. The tissue behind the mass can brighten, called enhancement, or darken, called shadowing. Shadowing behind a solid mass raises concern, since dense cancer tissue blocks the sound. The reader runs all five on each mass, then weighs them into a category. A few extra signs sit alongside the five. Calcifications inside a mass add to the worry, since the bright specks of cancer can sit within the tissue. Architectural distortion, a warping of the surrounding tissue with no clear mass, is a sign in its own right. A change in the skin or the nipple over a mass weighs heavily. These associated features do not replace the five. They push a borderline mass up a category. The reader also notes whether a finding is a single mass or one of many, since several similar masses in both breasts read as benign more often than a lone irregular one. The features carry unequal weight. A spiculated margin alone can push a mass to category 4 or 5, since few benign masses spiculate. A single benign feature does not clear a mass that carries a worrying one. The reader finds the worst feature and lets it set the floor for the category. A category built on the five features holds for the mass when the next reader checks it. A round, circumscribed, parallel mass with no shadowing reads as benign. A mass that is irregular and spiculated and taller-than-wide, with shadowing behind it, points to a likely cancer.
Orientation, the sign ultrasound owns
Orientation is the feature ultrasound brings that a mammogram cannot. A breast mass grows in a direction, and the direction means something. A benign mass, a cyst or a fibroadenoma, tends to grow along the tissue planes. It lies parallel to the skin, wider than it is tall. The growth follows the path of least resistance through the soft tissue.
A cancer grows another way. It pushes across the tissue planes, in whatever direction its cells take. The mass ends up taller than it is wide, standing up from the skin line. This taller-than-wide shape predicts cancer in around 71 percent of the masses that show it. Parallel orientation predicts a benign mass in around 78 percent. The two split from a single look at the mass.
The sign is read on a transverse image, with the long axis of the mass measured against the skin. A borderline mass, neither clearly parallel nor clearly tall, gets the benefit of the other four features. Orientation is strong. It stands with the rest, one feature among five, never the whole call on its own.
Orientation never stands alone.
A tall mass with a clean circumscribed margin can still be a benign fibroadenoma. A parallel mass with a spiculated edge is read as a cancer until proven otherwise. The shape is read with the features beside it, since the same orientation shifts in meaning between a clean edge and a ragged one.
Margin and posterior features
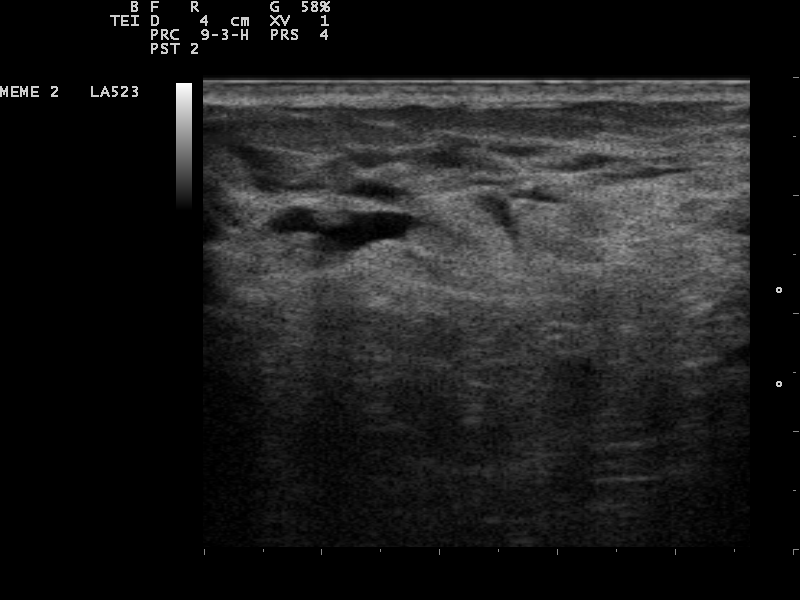
Small anechoic foci in the breast, the black of simple cysts. A cyst with a clean margin and posterior enhancement reads as a benign BI-RADS 2. Image: Nevit Dilmen, CC BY-SA 3.0, Wikimedia Commons.
Margin and posterior features carry the heaviest weight toward cancer. A circumscribed margin, a clean line around the whole mass, fits a benign lump. Around 90 percent of masses with a fully circumscribed margin are benign. The margin has to be clean all the way around. A single ragged edge breaks the benign call.
A spiculated margin marks the danger end. Sharp lines radiate out from the mass into the tissue, the look of a cancer reaching into the breast around it. A spiculated margin predicts cancer in around 91 percent of masses, the strongest single sign in the lexicon. Microlobulated and ill-defined margins fall between the clean and the spiculated, each raising the category a step.
Posterior features read the sound behind the mass. Enhancement, a bright zone behind a mass, marks fluid or loose tissue that lets sound through, often a benign cyst. Shadowing, a dark zone behind a mass, marks dense tissue that blocks sound, often a hard cancer. The posterior look adds to the read, since it reflects what the mass is made of, more than how its edge appears.
Two more boundary signs round out the read. An abrupt boundary, a sharp line between mass and tissue, fits a benign lump. An echogenic halo, a bright rim around the mass, or a thickened skin over it adds to the concern. The reader takes the whole back-and-edge picture together with the margin, since a mass can hide a worrying margin behind a calm posterior look.
How the features predict cancer
The lexicon is not a guess. Each feature carries a measured predictive value, drawn from large series of biopsied masses. The benign signs are strong. A circumscribed margin predicts a benign mass in around 90 percent. An oval shape predicts benign in around 84 percent. A parallel orientation predicts benign in around 78 percent.
The malignant signs are stronger still. A spiculated margin predicts cancer in around 91 percent. A taller-than-wide shape predicts cancer in around 71 percent. The reader stacks the features, since a mass with several malignant signs carries a higher risk than any one sign on its own. A clean mass with one worrying feature still warrants a closer look.
The numbers feed the category. A mass with every benign sign and no malignant one lands in category 3, watched with follow-up. A mass with a spiculated margin lands in 4c or 5, sent to biopsy. The category is the reader’s summary of the features, weighted by what each one predicts. A reader who knows the predictive values reaches a category that the next reader can trust.
The values hold up best when readers agree on the features. Studies of the lexicon find good agreement on shape and orientation. Agreement on margin runs weaker, where a ragged edge is a matter of degree. A center that trains its readers on the same lexicon narrows the spread and makes the categories hold from one reader to the next.
Ultrasound and mammography together
Ultrasound does not replace the mammogram. The two work together. A mammogram covers the whole breast and catches the fine calcifications that mark some early cancers. Ultrasound sorts a mass into solid or cystic and reads the dense breast that the mammogram cannot see through.
The dense breast is the place ultrasound was built for. Dense tissue reads white on a mammogram, the same white as a cancer, so a tumor hides in the crowd. Ultrasound reads through the density and finds a mass the mammogram missed. For a woman with dense breasts, an added ultrasound raises the number of cancers caught early.
On calcifications, the two tools trade strengths. A mammogram still leads for the faint specks of early cancer spread through the tissue. Ultrasound catches the calcifications inside a mass and adds the shape and the margin around them. The reader uses both, with the category drawn from the fuller picture the pair gives.
Supplemental ultrasound has moved into screening for dense breasts. Handheld scanning covers the breast in the reader’s hands. Automated systems sweep the whole breast in a set of stacked images for later reading. Both add cancers beyond the mammogram in dense tissue. The downside is more benign findings sent for a second look. A dense breast also raises a woman’s own risk, which makes the added scan a fair trade for the extra looks.
Reading BI-RADS on a handheld unit
A handheld unit runs the BI-RADS lexicon with a high-frequency linear probe. The reader scores shape, orientation, margin, echo pattern and posterior features on each mass, then assigns a category. The portable form carries the work to the bedside or to a clinic with no fixed imaging room.
Common questions about breast ultrasound BI-RADS
What does a BI-RADS category mean?
It is a number from 0 to 6 that sums up a breast finding and sets the next step. Category 1 is normal and 2 is benign. Category 3 is probably benign with follow-up. Categories 4 and 5 go to biopsy. Category 6 is a proven cancer.
What is the difference between BI-RADS 3 and 4?
Category 3 is probably benign, with a cancer risk under 2 percent, followed with a short-interval scan. Category 4 is suspicious, with a risk from 2 to 95 percent, sent to biopsy. Category 4 splits into 4a, 4b and 4c to grade the level of concern.
What features does ultrasound use for BI-RADS?
Five features: shape, orientation, margin, echo pattern and posterior features. The reader scores each one on a mass and weighs them into a category. Orientation, parallel or taller-than-wide, is the feature unique to ultrasound.
What does taller-than-wide mean?
It describes a mass that stands taller than it is wide, growing across the tissue planes. The shape predicts cancer in around 71 percent of masses that show it. A parallel, wider-than-tall mass is usually benign.
Why is ultrasound used with mammography?
Ultrasound sorts a mass into solid or cystic and reads the dense breast that a mammogram cannot see through. A mammogram leads for fine calcifications. The two work together for a fuller picture.
Can a handheld ultrasound assign a BI-RADS category?
Yes, with a high-frequency linear probe. It scores the same five features and assigns the same categories as a cart system, at the bedside or in a clinic without a fixed imaging room.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.