Lung Consolidation Versus Pulmonary Edema Ultrasound Differentiation
Two patients arrive short of breath, both with wet-sounding chests, both with white lungs on the screen. One is drowning in fluid backed up from a failing heart. The other has a lobe packed solid with the pus and debris of pneumonia. The first needs the water pulled off and the heart eased; the second needs antibiotics and time. The diuretic that saves the first would only dry out and harm the second. The probe is asked to tell these two apart at the bedside. It can, since the flooded lung and the consolidated lung carry different signatures to anyone who has learned to read them.
Same breathlessness, opposite cure.
The signs that separate them are plain once named. Edema spreads even and wide; consolidation sits focal and solid. Edema leaves the pleural line smooth; consolidation tears it ragged. Edema fills the lung with vertical lines; consolidation turns a patch of lung into something that looks like liver. The reading is a matter of pattern, distribution and a few bold marks, each learned in an afternoon and checked in seconds.
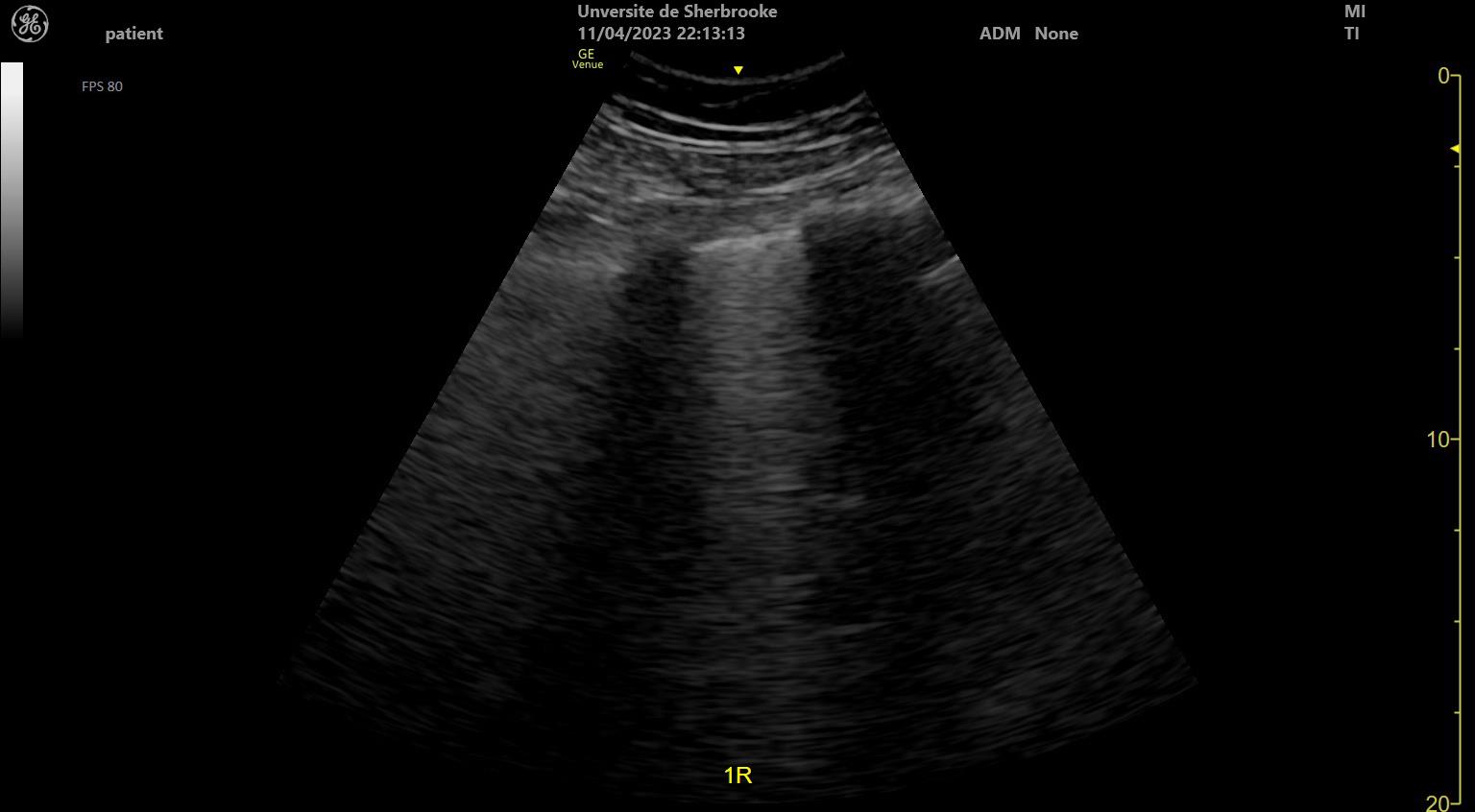
Consolidation versus cardiogenic edema. Left: a liver-like block with bright air bronchograms and a shredded deep edge. Right: even B-lines from a smooth pleural line. Original illustration.
Two floods, one cannot be drained
The stakes ride on the difference. A clinician who treats every white lung as heart failure pours diuretics into a patient whose lobe is solid with infection, drying the blood and starving the kidneys while the pneumonia rages on untouched. A clinician who treats every white lung as pneumonia loads antibiotics into a flooded chest and waits for a fever that never comes, the failing heart filling the lung further with every hour the diuretic is withheld. The two diseases wear the same face at the door and demand opposite first moves the moment the door closes.
The probe answers before the slower tests return. A chest film blurs the two together into a haze of white that a radiologist may take an hour to parse. The ultrasound reads the lung directly, at the bedside, in the first minutes, sorting the even flood of a heart from the solid patch of an infection while the treatment still hangs in the balance.
Read the pattern with care. The right cure follows close behind.
The shape of the trouble
Distribution is the first and largest clue. Cardiogenic edema is a tide; a tide rises everywhere at once. It floods both lungs together, top to bottom and side to side, heaviest where gravity pulls the fluid down, fading as the probe climbs toward the front of an upright chest. The pattern is symmetric, the two sides telling the same story, the change smooth from one rib space to the next.
Consolidation is a stain. A stain sits where it falls. Pneumonia packs one region solid and leaves the lung beside it dry and aerated, the border between sick and well often sharp enough to mark with a fingertip on the screen. Find a solid patch with healthy lung a few centimetres away, the sides of the chest disagreeing. The even tide of a heart grows unlikely.
Even and bilateral leans toward the heart. Focal and one-sided leans toward an infection.
When the lung turns to liver
The surest mark of consolidation is the lung that stops looking like a lung at all. A healthy lung is full of air. Air turns ultrasound back at the surface, so the depths of a normal lung show nothing but the repeating artifact of total reflection. Pack that lung with the fluid, pus and shed cells of pneumonia and the air is driven out. A lung emptied of air carries sound the way soft tissue does. The probe, reaching into a consolidated lobe, suddenly sees structure where it should see only artifact: a grainy, mottled grey block with the exact texture of liver, which is why clinicians call the finding hepatisation, the lung gone to the look of an organ. Threaded through that grey block run bright branching specks and lines, the air still trapped in the small airways, lit up against the airless tissue around them; these are air bronchograms. Their behaviour decides a great deal. Watch them through a breath. If the bright flecks shimmer and shift with each inflation, dynamic air bronchograms, air still moving in and out of open airways, the diagnosis swings hard toward pneumonia, since a patent airway feeding a solid lobe is the picture of infection over collapse. If they sit dead still, static air bronchograms, the airway is blocked and the lobe has fallen airless behind it, a collapse from obstruction instead. The deep edge of the consolidation gives a last sign. Where the solid tissue meets aerated lung, the border is jagged, broken, fractured, since the disease eats into the lung unevenly: clinicians name this ragged edge the shred sign, or the fractal sign. A smooth deep border argues against pneumonia while a torn one confirms it. Put the marks together, the liver-like block, the branching bright airways, the shredded deep edge, and the consolidated lung announces itself past any doubt.
Hepatisation, air bronchograms, a shredded edge: the lung gone solid speaks plainly.
The even tide of edema
The flooded lung speaks a quieter, more uniform language. Fluid backing up from a failing heart seeps into the thin walls between the air sacs, the interstitium, before it ever fills the sacs themselves. Sound striking these fluid-thickened walls rings back as bright vertical streaks that fall from the pleural line to the bottom of the screen, the B-lines. In edema they stand thick and even across both lungs, a row of bright bars where a healthy lung shows none.
The tissue stays soft and intact beneath them. The lung is waterlogged, drowned in its own interstitial fluid, the air not yet wholly driven out. So the deep architecture of the lung holds: no liver-like block, no shredded border, no branching air bronchograms, only the even fall of vertical lines from a pleural line that stays smooth and thin.
Spared patches help confirm it. Cardiogenic edema often leaves small windows of normal lung between the flooded zones, areas where the A-lines still show through, a patchwork the steady tide of a heart leaves behind. A pool of clear fluid in the chest, a pleural effusion sitting in the deepest corner, rounds out the picture of a heart that can no longer hold its load.
Even vertical lines, smooth pleura, soft lung beneath: the chest is wet, the tissue whole.
Reading the pleural line
The thin bright line where chest wall meets lung carries its own verdict. In cardiogenic edema the pleural line stays smooth, regular, unbroken, a clean stripe with the even B-lines falling from it, since the disease lives in the deep interstitium and leaves the surface tidy.
B-lines on lung ultrasound. Old fibrosis throws the same vertical lines as a flooded heart, a chronic mimic the history must sort out. Tinss, Wikimedia Commons, CC BY-SA 4.0.
In pneumonia the pleural line frays. The infection reaches the surface and roughens it, thickening the line, breaking it into a ragged, interrupted edge, sometimes pocking it with tiny surface consolidations the size of a grain. A torn, thickened pleural line under a patch of B-lines points at an infective cause; a clean one under an even field points at the heart. The line is small on the screen, easy to skip past in the hunt for the showier signs in the depths, yet a few seconds spent reading its texture often settles the question before the deeper marks are even weighed.
The B-lines that mislead
B-lines belong to both, and that shared sign is the trap. A clinician who counts vertical lines and stops has not yet separated the two, since the flooded lung and the consolidated lung both throw them. The difference lies in how they fall and what surrounds them.
In edema the B-lines are diffuse and even, spread wide across both lungs, falling from a smooth pleural line over soft lung. In pneumonia the B-lines cluster, focal and lopsided, gathered around a solid patch or a frayed pleural segment, with normal lung close beside them. The same bright streak, read for its company, tells two different stories. A lone cluster over a frayed segment is an infection until the rest of the chest says otherwise; an even curtain across both sides is a heart.
Count the lines, then read the lung they fall over.
Where the two can blur
The split is rarely as clean in a real chest as in a teaching one. A patient can carry both at once, a pneumonia laid on top of a failing heart, the even tide and the solid patch sharing one set of lungs and muddying the pattern. The probe shows the louder finding and can fall quiet on the second, leaving a clinician to weigh the history and the bloods alongside the screen.
Other states ape the marks as well. A lung collapsed from a blocked airway hepatises and shows air bronchograms much as a pneumonia does, separated mainly by the still bronchograms of a collapse against the moving ones of an infection. A lung scarred by old fibrosis throws B-lines and roughens the pleura without any fresh flood at all, a chronic pattern that the history, more than the probe, must sort from an acute one.
The reading is strong, never alone. It is a fast first sort, weighed against the patient and the story they bring, sharpest when the clinician treats it as a pointer toward the answer instead of the answer itself.
Walking the difference, step by step
The sequence runs the same way each time. Begin by scanning both lungs, top and bottom, front and side. Read the distribution first. An even field of B-lines across both chests, symmetric and gravity-heavy, raises the failing heart at once. A solid patch with dry lung beside it raises the infection.
Look next at the patch itself if one is found. Does the lung turn liver-like, grainy and tissue-dense in the depths. Do bright branching air bronchograms thread through it. Do they shimmer with the breath. Is the deep border shredded and torn. Each yes weighs the scale toward pneumonia, the consolidated lobe declaring itself through its own bold signs.
Read the pleural line through it all. A smooth, thin, unbroken line with even lines falling from it fits the flooded heart; a thickened, frayed, pocked line under clustered lines fits the infection.
Check the deepest corner for a pool of clear fluid, the pleural effusion that so often shadows a failing heart. Look for the spared windows of normal lung that the even tide tends to leave.
Then step back from the chest and weigh what the lung has said against the patient lying there, the fever or its absence, the swollen legs or the productive cough, the history that tips a close call. The probe has narrowed the field to one of two opposite cures, and the clinician chooses with the screen and the bedside together.
What it changed
Before the probe, the white lung was a puzzle solved slowly. A breathless patient with a hazy film waited on the radiologist, the bloods, the response to a cautious trial of treatment, the diagnosis emerging over hours as the diuretic helped or failed and the fever rose or stayed away. The clinician hedged, gave a little of each, watched to see which way the chest turned.
The ultrasound put the answer at the bedside in minutes. The even tide of a heart and the solid patch of an infection separate on the screen before the first drug is chosen, sparing the patient the harm of a treatment aimed at the wrong disease and the hours lost waiting to find out. A puzzle that once took a morning to settle now settles in the time it takes to sweep a probe across a chest and read what it finds.
The deeper gain was confidence at the first look. A clinician who reads the two patterns cold no longer treats the white lung as a guess refined by trial, but as a question the probe can answer on the spot, the cure chosen early and aimed true, the breathless patient spared the slow road to the same answer that once cost a morning of waiting.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.