Pericardial Effusion Emergency Assessment With Handheld Ultrasound
The patient’s pressure is low, the neck veins stand full, the heart sounds arrive muffled through the stethoscope. That triad is famous, and it is also a late guest; it shows up complete only when the patient is nearly lost. The probe answers the question a stethoscope cannot answer in time. Is there fluid in the sac around the heart. Is that fluid squeezing the heart shut. A handheld scanner replies in the seconds before an arrest, at the bedside, with no wait for a scan down the corridor.
Fluid around the heart can kill fast.
It can also sit for months and trouble nothing at all. The distance between the harmless trickle and the lethal squeeze is invisible to a hand on the chest. It is plain to a probe set against it. Reading that distance is the whole skill.
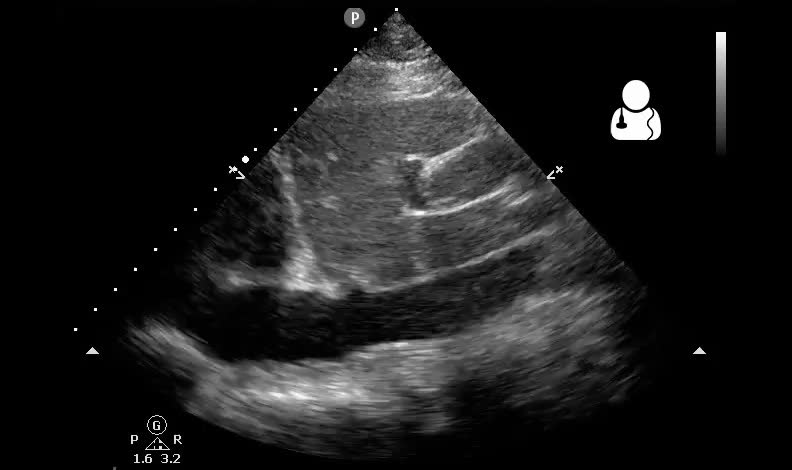
Pericardial effusion on bedside echo: anechoic fluid wraps the heart. Ultrasound of the Week / Wikimedia Commons, CC BY-SA 4.0
The sac and what fills it
The heart sits inside a tough fibrous bag, the pericardium, with a thin film of fluid easing the space between the bag and the muscle. A few millilitres is normal and silent. Disease tips far more into that space. Heart failure and kidney disease weep a clear fluid. Infection fills it with pus. A torn vessel or a ruptured chamber floods it with blood. The sac swells, the heart inside begins to feel the squeeze, the pressure climbs in a space that was never built to hold a flood.
The cause writes the tempo. A slow medical effusion can stretch the sac over weeks, letting it balloon to a litre or more before the heart complains. A fast bleed gives the sac no time to stretch. A few hundred millilitres, arriving in minutes, can close the heart down where a chronic litre beside it would not.
Black around the heart
On the screen the fluid reads black. Ultrasound paints it anechoic, a clean dark stripe or pocket wrapping the grey muscle of the heart. In a patient lying down the fluid pools where gravity sends it, behind the heart in the dependent space. A small effusion shows first as a thin dark line along the back wall. A large one surrounds the heart on every side, a black moat with the heart suspended in the middle of it. Where the dark space sits matters as much as that it is present. A stripe seen only in front of the heart raises the question of fat. A rim that wraps the back wall, deepening with each beat, is fluid, pooled where a lying body sends it. The eye that learns this dark rim catches the obvious effusion at a glance, long before any number is measured.
Why size is the wrong question
The instinct is to measure the effusion and grade the danger by its width. That instinct misleads more often than it helps, since the pericardium answers to pressure far more than to volume. The sac is a stiff bag with a steep pressure-volume curve. Stretch it slowly and it gives, accommodating a litre of fluid over weeks with the internal pressure barely rising; the heart fills normally through all of it, and a vast chronic effusion can leave a patient walking and well. Fill the same sac fast and the curve turns cruel. The bag has no time to stretch. Each added millilitre drives the pressure up a steep wall. A mere hundred or two hundred millilitres of fresh blood can lift the pressure inside the sac above the pressure inside the heart’s own chambers. At that moment the physiology of tamponade begins. The chambers do not all yield together. They collapse in the order of their own pressure, the weakest first. The right atrium, thin-walled and lowest in pressure, buckles inward at the end of its filling, when its own pressure sits at its lowest, pressed flat by the fluid outside it. As the sac pressure climbs further the right ventricle gives way too, caving in early diastole when it should be filling, a sign that carries more weight since the right ventricle is stronger and yields only under real strain. The heart, squeezed from outside, cannot fill from within. Less blood enters, less leaves, the stroke volume falls. The body answers with a racing pulse and clamped vessels, holding the pressure up by force. For a time it works. Then the compensation runs out, the squeeze wins, the output collapses, the patient arrests against a wall of fluid the heart cannot overcome. Speed, not size, decides which effusion does this.
Reading the squeeze
The probe reads the squeeze directly. The first sign sits at the right atrium, the chamber with the least pressure to resist the fluid. Late in the heart’s cycle, as the atrium relaxes, its free wall dimples inward, pushed in by the pressure outside. A brief inward flick is common and means little. A sustained inward buckling, lasting more than a third of the cycle, speaks of a sac pressure that has overtaken the chamber.
The second sign carries more weight. The right ventricle, stronger and thicker than the atrium, collapses only when the squeeze is real. Its free wall, watched in the moment it should be filling in early diastole, bows inward instead. A clinician who sees the right ventricle pressed in during diastole is watching tamponade happen, and reaches for treatment without waiting for the blood pressure to confirm what the heart already shows.
A swinging heart is the late, unmistakable sign.
The vein that confirms
One more window seals the read. The great vein returning blood to the heart, watched where it meets the liver, tells whether the circulation is dammed. In tamponade the heart cannot accept the blood arriving. The vein behind it swells and stays swollen, fat and motionless, refusing to collapse with the breath as a healthy vein does. A plethoric vein over a squeezed heart is the tank backing up behind a closed door, the confirmation that the dark space on the screen is doing real harm. A vein that collapses freely with each breath argues the other way, telling of a sac the heart still fills against, a finding that pulls a tense clinician back from the brink of an unneeded drain.
Telling pericardial from pleural
A black space near the heart is not always pericardial. A pleural effusion, fluid in the chest outside the heart’s sac, can sit close enough to fool the eye. The landmark that separates them is the descending aorta, seen in the long-axis view as a round vessel behind the heart. Pericardial fluid collects in front of the aorta, between it and the heart. Pleural fluid pools behind the aorta, further from the heart. The relationship to that one vessel sorts the two cleanly, even when the collections look alike.
The aorta is the dividing line.
Fluid around the heart on point-of-care ultrasound. Wikimedia Commons, CC BY-SA 3.0
The fat that fools
The other great mimic is fat. A pad of fat sits normally on the front of the heart, and on the screen it can read as a dark space that apes an effusion. Three things give it away. It sits in front of the heart only, never tracking around to the back where true fluid pools first. It is not purely black; it carries a grainy, speckled texture that pure fluid lacks. It moves with the heart wall instead of sitting still around it. A clinician who knows the fat pad is not fooled by a dark anterior stripe.
The trap runs the other way too. A clinician hunting an effusion can dismiss a real posterior collection as fat, or take an anterior fat pad as proof of fluid. The defence is to track the dark space around the heart and watch where it truly pools.
Where to put the probe
The heart offers more than one window. The choice depends on the patient. The subxiphoid view, taken from below the breastbone with the probe aimed up under the ribs, is the trauma standard. It shows the heart through the liver, the right-sided chambers nearest the probe, and a pericardial bleed shows clearly against the bright liver behind it.
The parasternal long-axis view, taken beside the breastbone, gives the cleanest look at the back wall where fluid pools first, and brings in the descending aorta that sorts pericardial from pleural. It is the window of choice when the subxiphoid view is poor, in a tense abdomen or a large body.
A clinician learns to switch windows the moment one fails.
The exam that came before
For a century the bedside had only indirect clues. Three signs, named together, pointed at tamponade: a falling blood pressure, a rising pressure in the neck veins, a quiet heart muffled by the fluid around it. The signs are real. They are also late and unreliable, arriving complete only in the patient already circling the drain, absent or partial in many who are dying all the same. An electrical tracing can hint at it. A chest film can show a swollen heart shadow. Neither sees the fluid.
The probe sees it directly. It does not infer the fluid from a blurred heart sound or a swollen shadow. It shows the black space itself, measures the squeeze on the chambers, reads the vein behind the heart. The indirect century ended the moment the sac appeared on a screen.
When the fluid must come out
When tamponade is closing the heart, the fluid has to come out, and ultrasound has changed how that is done. The old way was a blind needle pushed up under the breastbone toward the heart, guided by anatomy and hope. The probe replaced the hope with a picture. It finds the largest pocket of fluid, measures how deep it lies, marks the shortest safe path from skin to sac that misses the lung and the heart wall. The needle follows the route the probe drew, watched as it enters the black space and drains it.
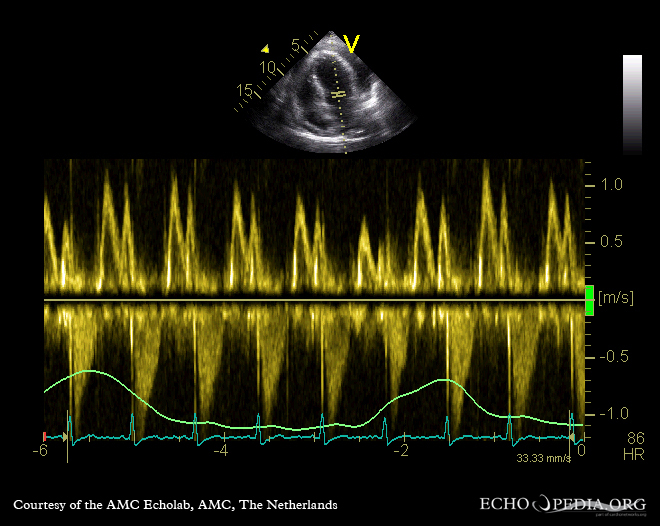
Mitral-inflow Doppler with marked respiratory variation, a hallmark of tamponade physiology. CardioNetworks ECHOpedia / Wikimedia Commons, CC BY-SA 3.0
Draining even a little can rescue a failing heart. The sac sits on the steep part of its curve. Letting out a small volume drops the pressure sharply. The chambers spring back open. A modest tap buys time the patient did not have.
What a clean look does not promise
A clear pericardium is reassuring, never a guarantee. A clot can sit in the sac after a stab or a rupture and read as grey tissue instead of black fluid, hiding a tamponade in plain sight. A loculated pocket behind the heart can fall outside a hurried window. A clinician reads a clean look against the whole patient, distrusts it when the pressure and the veins say otherwise. It scans again instead of standing down.
A film, never a snapshot
One look is a frozen moment. An effusion grows. A bleed that was a thin stripe on arrival can be a strangling moat twenty minutes on, and a heart that filled well at first can be buckling by the time the pressure drifts. Repeating the scan turns a single yes-or-no into a watch on a moving danger, at no cost beyond a minute and the probe already in hand.
Learning to read it
The first half of the skill comes fast. A black rim around the heart is a bold finding, caught within an afternoon of teaching, and the subxiphoid view that shows it is drilled into every trauma course. A learner spots a large effusion almost at once. The second half comes slower. Telling a fat pad from fluid, reading a subtle right-atrial collapse, judging whether a chamber is buckling under real pressure: these take hours at the probe and cases under a teacher’s eye.
The black space is easy. The squeeze takes practice to read.
What it changed
Before the probe, a pericardial bleed was a diagnosis made too late, confirmed on a table or at autopsy. The clinician facing a crashing patient guessed, treated blind, and learned the truth only when the chest was opened. Ultrasound put the sac on a screen. The same handheld carried for the trauma survey reads it, in the minutes that decide whether the heart keeps beating. The picture arrives early enough to act on, in the resuscitation bay, on the first pass of the survey, long before a cardiology review or a formal study could be arranged.
The deeper change is the question it reframed. The old question was how much fluid. The better one is whether the fluid is winning, read from the collapse of the chambers and the swelling of the vein, never from a measurement of width. A clinician who learns to read the squeeze stops grading effusions by size and starts seeing which ones are closing a heart.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.