Handheld Ultrasound Machine for Clinical Use Selection Criteria
A handheld ultrasound machine looks simple from the outside. The selection is anything but. Two probes that fit the same pocket can serve a clinic in completely different ways. The criteria below separate the device that earns its keep from the one that disappoints. Each criterion is a question the buyer should answer before the money moves.
A handheld earns its place by the picture it puts on the screen, then by everything that surrounds the picture.
Start with fit. Features come after.
A handheld is bought for a setting, a caseload, a pair of hands. The criteria are the lens that brings those three into focus. Read them in order. Skip none. The device that passes all of them is the one a clinic keeps reaching for a year later.
Criterion one: the clinical match
The first question is the plainest. Does the device scan what the clinic scans? A handheld built for cardiac work carries a phased-array head that slips between ribs. One built for vascular access carries a sharp linear head for shallow vessels. One built for the abdomen carries a curved head that reaches deep. A single probe rarely serves every job at full quality.
Match the head to the work first. Everything else is secondary.
A clinic that scans across areas faces a choice. It can buy several single-purpose probes. It can buy one wide-band probe that covers more of the range at some cost to peak quality. The right answer depends on the caseload. A focused practice does well with one well-chosen head. A general clinic needs breadth, even at a price. Naming the real caseload settles the question faster than any feature list.
Criterion two: image quality under real conditions
The findings that decide care are often subtle, and the device has to render them, not just the obvious ones.
Every vendor claims a clear picture. The claim means little until the device meets a real patient. Image quality on a handheld is a compromise. The small aperture and tight power budget cost some depth and some fine detail. The question is whether what remains answers the clinic’s question.
Test it on the hard cases. The easy ones flatter every device.
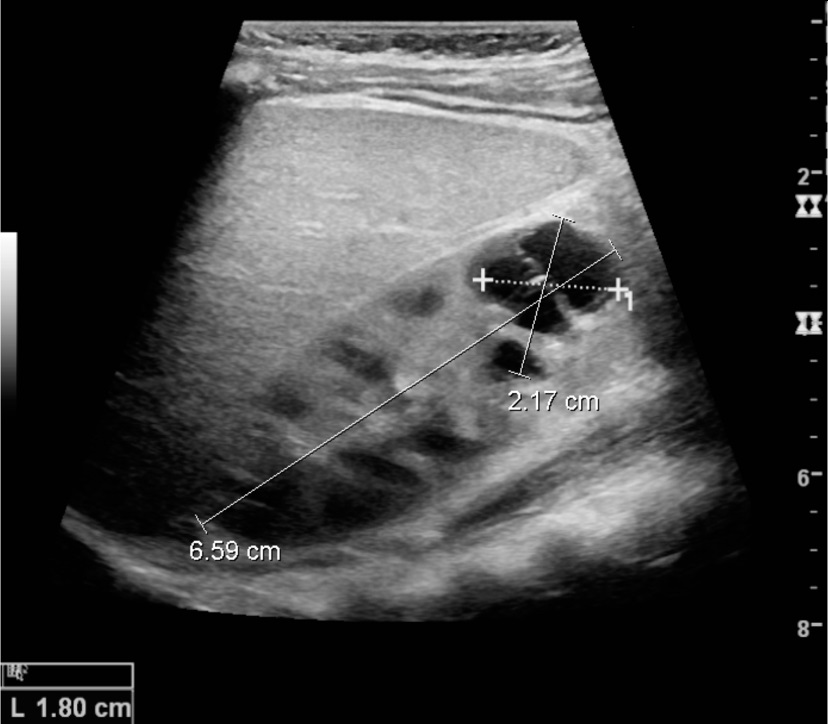
Resolution lives at the heart of this criterion, and it deserves a closer look than a single headline number allows. A handheld renders two kinds of detail. Axial resolution is the ability to tell apart two structures stacked along the beam, one behind the other. It improves with higher frequency and shorter pulses. Lateral resolution is the ability to separate two structures sitting side by side, across the beam. It depends on how tightly the device can focus the beam, which in turn depends on the size of the aperture and the cleverness of the electronics behind it. A small handheld has a small aperture. So its lateral resolution, especially deep in the body, falls behind a full system with a large probe. This is the gap a buyer feels on a difficult scan. A shallow vessel a centimetre down looks crisp on almost any handheld. A structure eight centimetres deep, in a large patient, separates the good devices from the cheap ones. The cheap one smears two close structures into one blur. The good one holds them apart. No spec sheet captures this well, because the headline frequency describes the probe, not the picture it makes at depth. The only honest measure is a scan, on the kind of patient the clinic sees in practice, at the depth the clinic truly works. A device that passes that test has earned the criterion. One that dazzles only on a slim model in a quiet room has not.
Criterion three: the people who will use it
A handheld is only as good as the hand that holds it. The third criterion looks past the device to the team. Who will scan with it? How trained are they? A tool that demands an expert touch fails in the hands of a generalist. A tool that guides a novice through a sweep extends what a clinic can do.
Buy for the team you have. The team you wish for is no help here.
Look at the interface. Count the taps it takes to reach a common mode. A device that buries color flow three menus deep slows every scan. Look at the guidance features. Some handhelds now coach the user toward a standard view, or flag a finding for a second look. In a clinic where scanning is a part-time skill, that help is the difference between a useful image and a guess. Match the device’s demands to the team’s training, and the purchase serves the work.
Criterion four: connectivity and the record
An image trapped on a device is half an exam. The fourth criterion asks where the picture goes. A handheld pairs with a phone, a tablet, or its own screen. Confirm the device works with the handsets the clinic owns. A probe that supports one brand and refuses another forces an awkward purchase down the line.
Then ask how the study leaves the device.
An exam belongs in the patient’s record. A device that exports over the standard medical-imaging protocol folds into the clinic’s systems. One that locks images in a private app creates friction at every step. Check the path from scan to record before buying. A clean path saves an hour a week that a clumsy one steals.
Criterion five: endurance and build
Color and spectral Doppler change what a handheld can answer, and they push the probe hardest.
A clinical day is long. A handheld has to last it. The fifth criterion covers battery and build. Read the scan-time figure with suspicion. Vendor numbers come from gentle modes. Real use, with color flow and frequent scans, drains a cell faster. A device that dies mid-list is a device half-trusted.
Then weigh the build against the clinic’s reality.
A handheld gets dropped. It gets wiped with strong disinfectant. Its scanning face meets gel and skin all day. A sealed, fluid-resistant body survives this. A flimsy one cracks, then leaks, then fails. Ask the rating. Ask what the cleaning agents do to the housing over a year. A device that cannot take the clinic’s cleaning routine is a device on borrowed time.
Criterion six: clearance and support
A medical device answers to rules. The sixth criterion confirms the device clears them. A handheld sold for clinical use must carry the clearance the clinic’s market requires. A grey-market unit, cheaper at the border, can fail an inspection and cost more than it saved.
Support is the criterion buyers forget.
A device with no local service is a device with a short life. When a probe faults, the clinic needs a fix in days, a wait of months is its own kind of failure. Ask where support sits. Ask how a repair is handled. A vendor with a presence near the clinic keeps the device running. One an ocean away leaves it dead on a shelf. The picture quality wins the demo. The support wins the years that follow.
Criterion seven: the whole cost
Price is the last criterion, and the easiest to misread. The number on the listing is rarely the cost. A bare probe with no warranty, no training, and a costly replacement part can outspend a dearer, complete package within a year. Build the full figure. Add the probes the caseload needs. Add the warranty. Add the training. Add a spare where one device is too few.
Compare the totals. The headline prices mislead.
A clinic that buys on the sticker tends to buy twice. A clinic that prices the working system tends to buy once. The criterion is met by the device whose true cost, across its working life, makes sense for the work it does. The smaller number on the first page seldom wins that test.
What the warranty truly covers
A warranty is a promise with fine print. The headline says two years. The detail decides what those years are good for. The first question is the probe. On a handheld, the transducer is the device. A warranty that covers the body but excludes the probe covers the cheap part and leaves the dear one exposed.
Read what the warranty excludes. The claims always read better than the exclusions.
Drops are a common exclusion. So is fluid ingress, the one thing a clinical probe meets all day. A warranty that voids on the first accident, in a setting built on accidents, protects the vendor and not the clinic. Ask how a claim is handled. Ask whether a loaner arrives while the faulty unit is away, since a clinic with one scanner cannot pause for a repair. Ask who pays the shipping, which on a cross-border claim can rival the part. The warranty that matters is the one that keeps the clinic scanning through a fault. A policy that only reads well until the day it is needed is the wrong policy.
The upgrade question
A handheld is a smaller commitment than a cart. It is still a commitment of years. The seventh thing to weigh is what happens as the device ages. Software is the quiet half of a modern probe. A maker that ships new features to an existing device extends its life. One that abandons last year’s model the moment a new one ships shortens it.
Ask how long the device keeps getting updates.
A probe locked to a phone app inherits that app’s fate. When the app stops supporting the clinic’s tablet, the probe goes quiet, no matter how sound the hardware. A device tied to an open standard ages more gracefully. The upgrade question rarely surfaces in a demo. It decides whether a purchase serves three years or thirty months. A clinic that asks it early avoids the expense of a device that works while its software is fed, then dies the day the feeding stops.
Putting the criteria together
No single criterion decides the purchase. A device can ace image quality and fail on support. It can be cheap and clear no rules. The selection is the weighing of all seven against the clinic’s own facts. The clinical match comes first. The rest qualify and temper that match.
Score the device against each, then look at the whole.
A handheld that meets the clinical match, holds its picture on hard cases, suits the team, feeds the record, lasts the day, clears the rules, and prices honestly is the device to buy. One that stumbles on a criterion the clinic cares about is the device to pass over, no matter how bright its brochure. The criteria do not pick a brand. They pick the fit. A clinic that runs them in order buys a tool it keeps, and skips the regret that follows a purchase made on a headline alone. The order itself carries a lesson. Image quality tempts a buyer first, since it is the part a demo shows off. The criteria that decide a device’s long life sit lower on the page: the support behind it, the warranty that holds through a fault, the path that carries a study into the record, the updates that keep it current. A clinic that lets the bright picture settle the purchase often meets the quieter criteria too late, on the day a probe faults and the phone goes unanswered.
The handheld that serves a clinic for years is rarely the one that won the showroom. It is the one chosen against the full list, with the dull criteria weighed as heavily as the dazzling ones. That discipline is unglamorous. It is also the difference between a device on the bench and a device in a drawer.
The criteria reward patience.
A buyer who walks the full list spends an afternoon that a hasty purchase would have skipped. That afternoon is cheap against the cost of a wrong device: the months of a probe that smears the scans, the inspection that flags a missing clearance, the silence of a vendor who cannot be reached. The clinic that scores a handheld against every criterion, then trusts the total over the brochure, buys once and scans for years. The work it does, quietly and daily, is the only verdict that lasts.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.