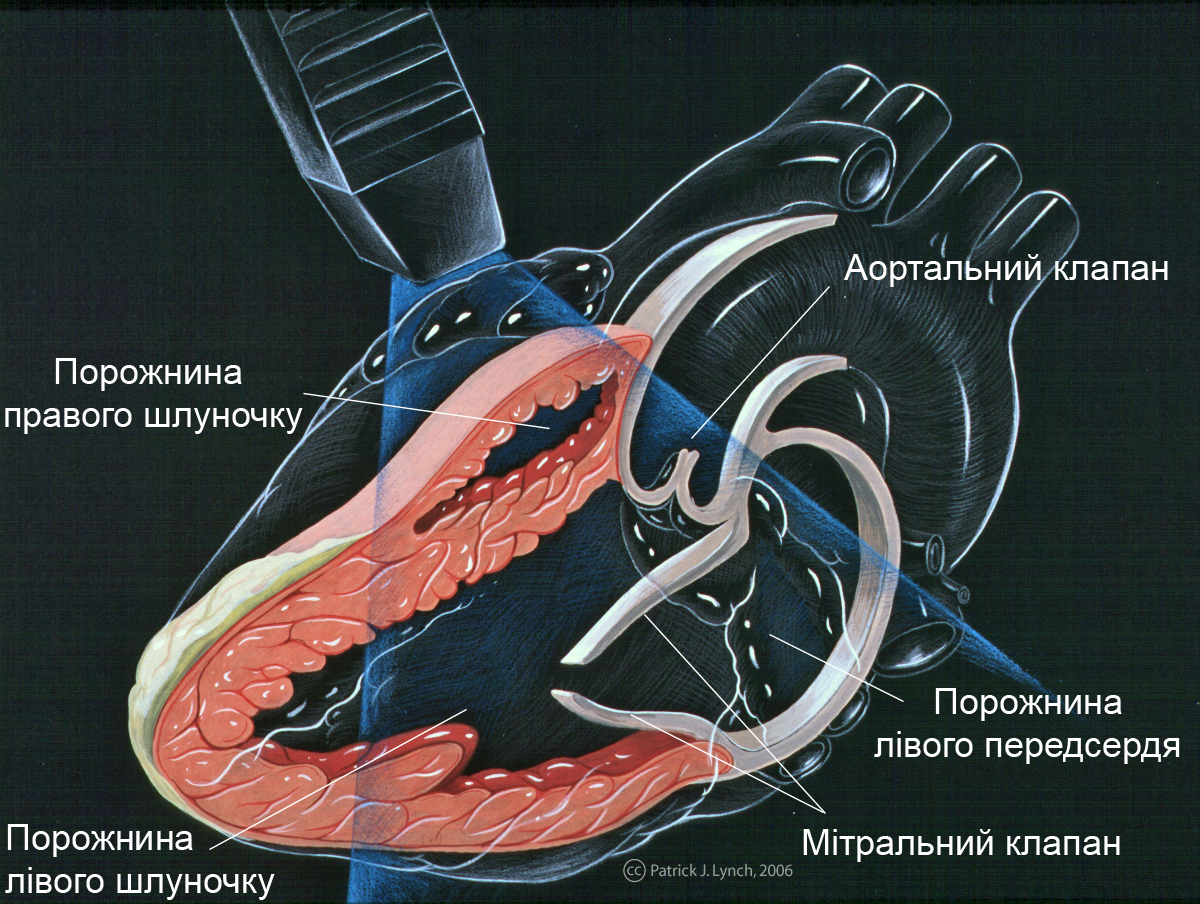
An echocardiographic view; the beating heart is read in its motion, which a smooth frame rate preserves and a stutter destroys.
Frame rate is the number of images an ultrasound probe paints each second, and the figure of twenty-four frames a second carries a particular meaning, since it is roughly the rate at which a sequence of stills stops looking like a slideshow and starts looking like motion. It is the rate cinema settled on for the same reason, the point where the eye fuses separate frames into smooth movement, and for point-of-care ultrasound, where the clinician is usually watching something move, that smoothness is not a comfort but a diagnostic tool. A heart contracting, a vessel pulsing, a lung sliding, a needle advancing toward a target, all of these are read in their motion, and a probe that cannot hold a smooth frame rate turns living movement into a stutter that hides exactly what the clinician came to see. The twenty-four figure is a floor that rewards understanding, and the honest question is never the peak frame rate but the rate the probe holds at the depth and mode the work genuinely uses.
Below smooth motion a scan is a slideshow, and a slideshow hides the very thing a moving study is meant to show.
Why motion is the point in POCUS
Point-of-care ultrasound is often less about a single still picture than about watching how something behaves over time, and that focus on movement is what makes frame rate matter more here than in a study read from frozen images.
A clinician assessing the heart is judging how the walls move and how the chambers fill and empty, a question that only motion answers, so a stuttering image that drops the moments between frames can hide a wall that moves poorly or a valve that closes wrong. Watching the lung, the clinician looks for the shimmer of the surfaces sliding against each other with each breath, a subtle motion that a low frame rate can smear into stillness and lead to a missed or false finding. Guiding a needle toward a target, the operator needs the tip to move on the screen the instant the hand moves, since a laggy or stuttering image makes a fine, careful advance into a guess. In each of these the information lives in the change between frames, and a probe that paints too few frames a second simply throws away the moments where the diagnosis hides, showing a series of disconnected snapshots where a smooth sequence was needed. This is why frame rate is a clinical specification in point-of-care work and not a matter of how pleasant the image looks, since the smoothness is the means by which motion is read, and a study that should be watched in real time loses its meaning the moment the picture begins to jump.
What moves is what matters, and a probe that stutters loses the motion the clinician was reading.
What the twenty-four figure does and does not promise
The twenty-four-frame threshold is a useful landmark and a partial one, since it marks where motion begins to look continuous but does not guarantee that every moving structure is captured faithfully.
Fetal scan frames; below smooth motion a moving study becomes a series of disconnected snapshots.
At roughly twenty-four frames a second the eye stops seeing separate stills and perceives smooth motion, so a probe that sustains that rate or better shows movement a clinician can follow rather than a flickering sequence, and this is the real meaning of the figure as a floor. It is a floor and not a ceiling, since some structures move fast enough that even smooth-looking motion at twenty-four frames blurs the quickest events, and a rapidly beating heart or a fast valve can ask for a higher rate to be read in full, so twenty-four is the minimum for comfort rather than the optimum for every task. The figure also says nothing on its own about the conditions it was measured under, since a probe can hit a high frame rate at a shallow depth over a narrow field with no colour flow and fall far below twenty-four when the depth increases, the field widens, or a colour mode is switched on. A clinician scanning deep or running colour flow may find the same probe that looked smooth on a shallow grayscale sweep stuttering badly under the real settings, so the headline frame rate without its conditions is a best case rather than a working figure. The twenty-four-frame mark is meaningful as the line below which motion breaks up, and useful only when a buyer asks at what depth, width, and mode the probe stays above it, since a probe that clears it only in the easiest setting has cleared it where the clinician needed it least.
Twenty-four frames is the floor where motion turns smooth, not the ceiling every fast structure needs.
What frame rate trades against
Frame rate is not a free quantity a maker simply chooses, but the result of a hard trade against depth, field width, and imaging mode, all bound by the fixed speed of sound in tissue.
Every line of the image is made by sending a pulse and waiting for its echo to return from the depth, and since sound travels at a fixed speed, a deeper scan makes each line take longer, so depth and frame rate pull against each other directly. A wider field needs more lines to fill it, and more lines at a given depth take more time, so widening the view lowers the frame rate just as deepening it does. Colour flow is the heaviest cost, since building a colour image takes several pulses per line where grayscale takes one, so switching on colour can halve the frame rate or worse, and a probe that looked smooth in plain grayscale can stutter the moment colour is added. The channel count enters here too, since a probe that can form several receive lines per pulse gathers the image faster and holds a higher frame rate at a given depth and width, and beamforming hardware and frame rate are linked for that reason. The frame rate a probe achieves is, in the end, the outcome of all these factors together, and a single quoted number means little without the depth, the width, and the mode it was measured at, since the same probe delivers very different rates across the settings a real day uses.
Where a higher rate earns its place
If twenty-four frames is the floor for smooth motion, it helps to know where a rate well above it changes a diagnosis and where it adds nothing a clinician can use.
The fastest-moving structures set the real demand, and the heart is the clearest case, since a valve can open and close in a fraction of a second and a wall can move quickly enough that twenty-four frames blur the very moment a clinician wants to see, so cardiac work rewards a frame rate well above the floor. Fine procedural guidance benefits too, since a needle advanced in small deliberate movements is easier to track when the screen updates many times a second, and the extra frames make the tip’s motion feel immediate rather than caught up to. For slower questions, the size of an organ, the presence of fluid, a static measurement, the motion barely matters and any rate above the floor serves equally, so the headline frame rate idles on work that does not move. The point is that the right frame rate follows the speed of what is being watched, and a clinic doing fast cardiac work needs headroom above twenty-four that a clinic measuring static structures does not, so the figure should be matched to the fastest task the probe will face rather than admired in the abstract. A maker that asks what the buyer scans can say whether the frame rate matters greatly or barely, while one that quotes a single high number leaves the buyer to guess whether it survives their settings. The faster the anatomy, the more the frames above the floor earn their keep.
The quick heart wants frames to spare; the static measurement is content with the floor.
The whole chain behind a smooth picture
Frame rate is best understood as the visible end of a chain that runs from the beamforming hardware through the processing to the screen, since a weakness anywhere in that chain shows up as a stutter the clinician feels.
The beamformer sets how fast lines can be gathered, the channel count deciding whether several receive lines come from each pulse, so the hardware fixes the ceiling on frame rate at any given depth and width. The processing that turns echoes into a picture has to keep pace, since a frame gathered quickly is of no use if the device cannot render it in time, and a probe with fast acquisition but slow processing stutters despite its hardware. The wireless link carries the finished frames to the screen, and a link that drops or delays frames undoes the frame rate the probe worked to achieve, so a smooth acquisition can still arrive at the phone as a stutter if the radio cannot keep up. The display itself has a refresh limit, though it rarely binds before the other stages do. A clinician who sees a stuttering image cannot tell from the screen which link failed, the beamformer, the processing, or the radio, and only knows that the motion broke up, and the honest test is to watch real motion end to end rather than to read any single number. Frame rate is the symptom that reveals the health of the whole imaging chain, and a probe that holds a smooth picture at clinical settings has every link of that chain working together.
A smooth picture is the whole chain succeeding at once, and a stutter is the weakest link confessing.
What the buyer should weigh
Frame rate is one of the more honest specifications when its conditions are stated and one of the more misleading when they are not, so the buyer has to ask for the conditions and test under the real ones.
The first move is to ask at what depth, field width, and mode the quoted frame rate was measured, since a peak figure at shallow narrow grayscale tells little about the rate the probe holds during a deep scan with colour flow running. The second is to test the probe on the kind of motion the work involves, watching a beating heart or a sliding lung at the actual clinical settings rather than a still phantom, since only moving anatomy reveals whether the frame rate holds where it matters. The third is to switch on colour flow and see how far the rate falls, because the drop is steep and a probe that stays smooth in grayscale can become a slideshow in colour. The fourth is to relate the frame rate to the channel count and processing, since those decide whether the probe can hold a usable rate at depth or only at the surface. A buyer who watches real motion at real settings, with colour on, has tested the frame rate the way the work will, while one who reads the peak figure has trusted the best case the maker chose to print. Watch the motion at the settings you will use, with colour running and the depth the work demands, and the frame rate tells the truth a single number printed on a box never can.
The peak frame rate is the easy boast; the rate the probe holds on moving anatomy at clinical settings is the one that reads the diagnosis.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.