A color Doppler scan; an electromagnetic disturbance that corrupts such an image is the hazard this standard guards against.
IEC 60601-1-2 is the standard that asks whether a medical device can survive the electromagnetic noise of the real world and whether it adds too much noise of its own. Every powered device both emits electromagnetic energy and is vulnerable to the energy around it, and a hospital is one of the noisiest electromagnetic environments there is, full of motors, radios, phones, diathermy, and a hundred other devices all radiating at once. This collateral standard, sitting beside the general electrical safety standard, governs two halves of one problem: emissions, that the device must not throw out interference that disrupts the equipment around it, and immunity, that the device must keep doing its job, or fail in a safe and obvious way, when the interference comes the other direction. For a wireless ultrasound probe, which intentionally broadcasts a radio signal and is meant to work in ambulances, clinics, and homes rather than a shielded room, this standard is unusually demanding.
A probe has to be a quiet neighbour and a tough one at the same time.
Two directions, one problem
The standard splits cleanly into the energy a device sends out and the energy it has to withstand. Both matter, and a device can be excellent at one and dangerous at the other.
On the emissions side, the device is limited in how much electromagnetic energy it may radiate or conduct back into the mains, since a device that floods its surroundings with noise can corrupt the readings of a monitor beside it or the signal of another device sharing the room. On the immunity side, the device is bombarded with the kinds of disturbance it will meet in service, a strong radio field, a static discharge from a touch, a fast transient on the power line, a surge, a magnetic field from a nearby source, and it has to come through each without losing what the standard calls its essential performance. Essential performance is the part that has to keep working for the device to be safe, and for an imaging probe it is the production of an image that can be trusted, free of artefacts that could be read as anatomy and with measurements that stay accurate. The standard is precise that immunity does not always mean uninterrupted operation, since a device that detects a disturbance, flags it, and recovers can be safe, while one that quietly produces a corrupted image during interference is dangerous in a way that is hard to catch. The two directions are tested separately and judged together, and a probe has to pass both to earn the conformance.
Emitting little and enduring much are different skills, and a device needs both.
What the immunity tests throw at a device
The immunity half is a battery of deliberately hostile tests, each standing in for a real disturbance the device will meet, and the list rewards knowing because it maps onto the hazards of real use.
An abdominal scan; essential performance for a probe is an image free of artefacts that could be read as anatomy.
A radiated radio-frequency field test bathes the device in the kind of signal a mobile phone or a two-way radio puts out at close range, since those are exactly what a clinician carries and what sits in an ambulance, and the device has to keep imaging through it. An electrostatic discharge test zaps the device with the static a person builds up walking across a floor and discharges on touch, a daily event the housing has to absorb without the electronics faltering. Electrical fast transient and surge tests hit the power and signal lines with the spikes that switching equipment and lightning induce, and conducted immunity tests inject disturbance directly into the cables. A magnetic field test exposes the device to the fields near power equipment and, in the current edition, to the proximity fields of wireless power and radio-frequency identification readers that a portable device now meets in the wild. Each test has a defined level, and the level is not the same everywhere, since the standard sets higher immunity requirements for devices used in the home and field environment than for those confined to a professional healthcare facility, on the reasoning that an uncontrolled environment subjects a device to worse and less predictable interference. A probe meant to leave the hospital has to clear the harder bar, and a maker that tested only to the professional level has certified a device for a gentler world than the one it will live in.
Each test is a rehearsal for a disturbance the device will truly meet in a clinic or an ambulance.
Essential performance is the heart of it
The phrase essential performance carries more weight in this standard than any test level, since it defines what the device has to protect when the interference arrives.
A maker has to decide, and justify, what its device must keep doing to remain safe, and for an ultrasound probe that is the delivery of an image and measurements a clinician can rely on. The standard then asks whether each immunity test leaves that essential performance intact, and the dangerous failure is not the device that freezes or reboots, which an operator notices at once, but the device that keeps showing an image while the interference quietly distorts it. An artefact induced by a radio field that looks like a shadow in tissue, a measurement that drifts because a disturbance corrupted the calibration, an index on the screen that no longer reflects the true output, these are the failures the standard is built to catch, because they mislead rather than alarm. A maker that has thought clearly about essential performance designs the device to detect such corruption and warn the operator, or to degrade in a visible way, rather than to soldier on producing a confident wrong picture. The whole point of tying immunity to essential performance is that safety is not the device merely surviving but the device not lying, and a probe that goes on imaging through interference without flagging the corruption has passed a crude test and failed the real one. Reading an EMC report well means reading how essential performance was defined and whether the hard failure modes were the ones the maker looked for.
What the wireless handheld makes harder
A wireless handheld probe is an unusually difficult case for this standard, because it is at once a deliberate radio transmitter and a device meant for the least controlled environments.
The probe broadcasts an image over a radio link, which means it is an intentional emitter that has to coexist with every other radio in a crowded band without either jamming its neighbours or being jammed by them, a coexistence problem a cabled probe never had. It is also designed to leave the shielded calm of a radiology suite and work at a roadside, in an ambulance bouncing with two-way radios, or in a home full of consumer electronics, exactly the home and field environment for which the standard sets the higher immunity bar. The small sealed body that makes it portable leaves little room for the shielding and filtering that a large cart could hide inside its chassis, so the maker has to win its electromagnetic robustness through careful design rather than brute mass. A handheld that drops its radio link under a moderate field, or shows artefacts when a phone rings beside it, has failed in precisely the conditions it was sold to handle, and the failure is invisible until it happens to a patient. A maker confident in its engineering tests to the field-environment levels, defines essential performance honestly, and shows that the device fails safe rather than fails silent, while one that cut the work tests to the easier professional level and hopes the field is gentle.
The device built to broadcast and to travel meets the worst electromagnetic conditions and has to be designed for them, not excused from them.
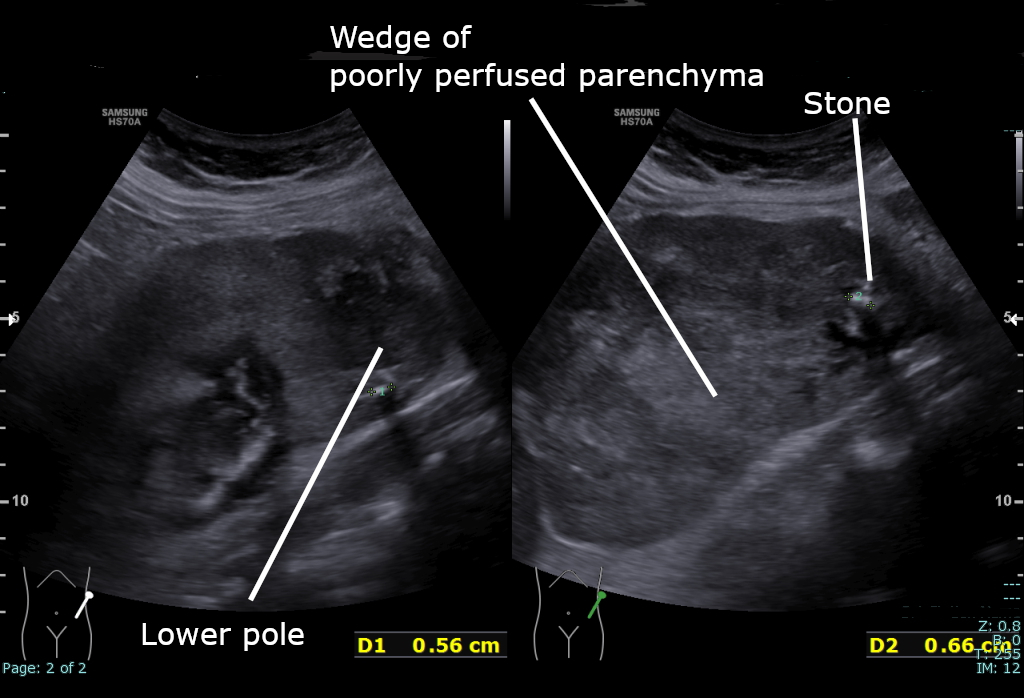
A renal scan; a stray radio field must not quietly paint a shadow a clinician mistakes for a lesion.
How it sits among the safety standards
Electromagnetic compatibility is not a free-standing concern but one control in the larger safety case, and seeing where it fits explains why a probe needs it however clean its acoustic output looks.
In the language of the risk management standard, an electromagnetic disturbance is a hazard like any other, and conformance to this standard is the control measure that answers it, the evidence the risk file points to when it claims the device behaves safely amid interference. The general electrical safety standard governs the device on its own bench, the particular standard for diagnostic ultrasound caps and displays the acoustic output, and this collateral standard governs how the device behaves when the world around it is electrically loud, so the three describe the same device from three angles that have to agree. A probe can clear its acoustic limits perfectly and still be unsafe if a passing radio field paints an artefact the clinician reads as a lesion, and that is the reason the imaging integrity that the acoustic standards protect at the source has to be protected again here against corruption from outside. The wireless link adds a further thread, since the radio that carries the image is governed both by this medical standard and by the general radio regulations of each market, and a maker has to satisfy both without letting either undermine the other. A reviewer reading the whole file checks that the essential performance named in the EMC work is the same imaging integrity the acoustic and risk documents protect, since a probe whose documents disagree about what matters has not been thought through as one device. The standard earns its place by guarding the one thing all the others also guard, the reliability of the picture, against a threat the others do not address. A buyer who sees the EMC conformance listed alongside the acoustic and electrical ones is seeing a maker that closed the last common door into the image, and a file that names every other standard but skips this one has left that door open.
Clean output means nothing if a stray field can quietly rewrite the picture, and this standard is what stops it.
Reading an EMC report
A buyer does not have to understand field strengths to tell a thorough EMC qualification from a thin one, and a few questions separate them.
The first is which environment the device was tested for, since a probe meant to leave the hospital should be qualified to the home and field levels rather than the professional ones, and a report that quietly used the gentler levels has certified the device for the wrong world. The second is how essential performance was defined, because a definition that names the image and the measurements as the things to protect is one that took the real hazard seriously, while a vague definition lets a maker pass without confronting the failure that matters. The third is whether the report covers the device as it genuinely ships, radio active and running, rather than a quieted-down sample, since a probe tested with its wireless link disabled was tested as a different device. The fourth is whether the failure modes were the misleading kind the maker looked for and guarded against, rather than only the obvious freezes. A report that addresses these reads as the work of a maker that understood the electromagnetic life its device would lead, since the maker had to picture the ambulance and the crowded ward to test for them, and a probe whose EMC was taken seriously is one a clinician can trust to either work or say plainly that it cannot, which is all immunity ever promises.
The probe a buyer should trust either keeps imaging honestly through the noise or tells the operator it cannot, and never quietly does neither.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.