TTE Transthoracic Echocardiography Five Standard Views Handheld
The heart hides behind the ribs and the lung, a moving target wrapped in bone and air that turn ultrasound away. A full echocardiogram hunts it from a dozen angles over half an hour. The focused exam, the kind a handheld probe runs at the bedside, asks for only five. Five windows, each a gap in the bone and air through which the heart shows itself, are enough to answer the questions that decide the first minutes of care: is there fluid around the heart, is the muscle pumping, is the right side strained, is the tank full or empty. A clinician who can find those five windows can read a frightened heart in the time it takes a full study to begin.
Five windows, four questions, one quick answer.
The skill is in the hands more than the head. Each window has a spot on the chest, a tilt of the probe, a turn of the marker; once those are drilled the heart appears where it should, the same way on every patient. The reading that follows is the easy part; the finding of the window is the craft.
The five views come from three spots: the left parasternal edge (long and short axis), the apex, and below the breastbone (four-chamber and the vena cava). Original illustration.
Why five and not the whole heart
A comprehensive echo is a specialist study, long and thorough, mapping every valve and wall from every angle. It answers questions a focused exam never asks. The bedside scan trades that depth for speed, taking the few views that catch the findings which change what happens next, leaving the fine detail to the cardiologist and the cart-based machine.
The five views are chosen for coverage, not completeness. Between them they see all four chambers, the great vessels leaving the heart, the sac around it, and the big vein feeding it back. A problem large enough to matter in a crashing patient shows itself in at least one of the five, which is why the set is built the way it is: the smallest number of windows that still leaves nowhere big for trouble to hide. A pinhole leak in a valve or a single wall that moves poorly can still slip past all five; the focused exam was never built to catch the fine faults, only to seize the large, fast killers that a slow study would reach too late.
Speed is the whole point.
The marker and the screen
Every view turns on two things: where the probe sits and which way its marker points. A small notch on the side of the probe maps to one edge of the screen, so the orientation of that notch decides which way the heart is drawn. Cardiac scanning keeps its own convention for that mapping, a mirror of the one abdominal scanning uses. A clinician who mixes the two will read a heart flipped left for right.
Hold the convention steady and the windows line up. Learn where the marker points for each of the five, drill it until the hand turns there without thought; the heart arrives on the screen the same way every time, ready to read. Fumble the marker and the chambers land in the wrong corners, a normal heart made to look diseased by nothing more than a probe held backward. The guard against it is a habit more than a calculation: the marker turned to the same landmark for each window, checked before the image is read, so left stays left through all five.
The five windows
The set runs in a familiar order, each window found by hand from plain landmarks. The first is the parasternal long axis: the probe sits just left of the breastbone, in the third or fourth space between the ribs, its marker turned toward the patient’s right shoulder, and the beam slices the heart along its length, laying the left ventricle, the mitral valve, the aortic valve and a slice of the left atrium across the screen in one long view that reads pumping and valves at a glance. Turn the probe a quarter circle from there, the marker swung toward the left shoulder, and the same parasternal spot gives the parasternal short axis, a cross-section that cuts the left ventricle into a thick ring, a doughnut of muscle whose even squeeze tells the strength of the pump and whose shape betrays a right side under pressure. Slide the probe down and out to the point where the beat is felt strongest, near the fifth space below the left nipple, marker to the patient’s left, and the apical four-chamber view opens, the beam looking up through the apex to lay all four chambers side by side, the one window that sets the right ventricle against the left and asks whether the right is swollen. Drop the probe to the soft spot under the breastbone and lay it almost flat against the belly, aimed up under the ribs toward the left shoulder, and the subcostal four-chamber view climbs to the heart from below, a window that shines in a crashing patient since it needs no roll and survives the chest compressions of a resuscitation, the surest place to catch fluid in the sac. Keep the probe under the ribs but turn it upright, marker toward the head, and the last window finds the inferior vena cava in its long axis, the great vein running into the right atrium, its width and the way it collapses with a breath reading the fullness of the tank. Five spots, five turns of the hand, the whole heart sampled in a sweep that a trained hand runs in a couple of minutes.
Parasternal long, parasternal short, apical, subcostal, the vein.
What each window answers
The views earn their place by the questions they settle. The sac around the heart is read best from the subcostal window and the parasternal long, where a dark rim of fluid between heart and sac stands out at once; a large rim with a heart swinging inside it warns of tamponade, the squeeze that stops a heart from filling. A thin rim that sits quiet as the heart beats is the slower, chronic kind, watched instead of drained; the depth of the rim and the swing of the heart within it sort the urgent from the harmless.
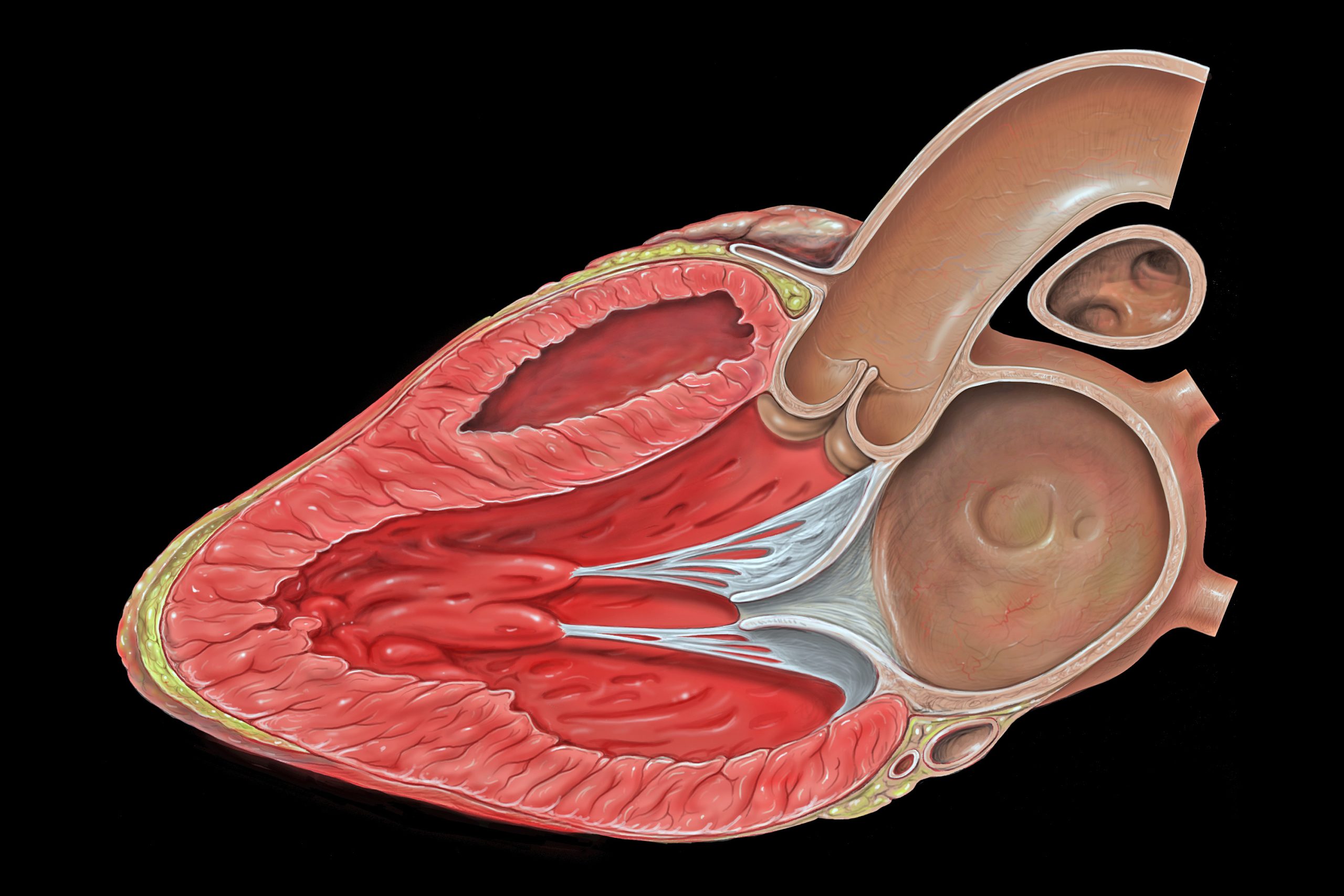
A parasternal long axis view: the left ventricle, mitral valve, aortic valve and left atrium in one slice. Patrick J. Lynch, Wikimedia Commons, CC BY 2.5.
The strength of the pump reads from the parasternal and apical windows together. The eye watches the left ventricle squeeze, the walls thickening and the cavity shrinking with each beat. It judges the pump strong, fair or failing without a single measurement, an eyeball estimate that a focused exam leans on hard. A heart that barely stirs, its walls slack and its cavity wide, marks a failing pump that wants support; a small chamber squeezing down to nothing marks a tank run dry, the muscle strong but starved of volume.
The right ventricle tells its own story in the apical and short-axis views. A right ventricle as big as the left, or bigger, bulging against the septum and bowing it into the left, points at a sudden strain on the right side, the picture a large clot in the lungs can paint. The healthy right ventricle sits smaller than the left, a slim crescent hugging its flank; when it swells to match or overtake the left, the change is plain to an eye that holds the normal proportion in mind.
The vein answers the question of volume. A wide vena cava that barely budges with a breath says the tank is full, the pressure high; a narrow one that collapses with each breath says it is empty, a body that may take more fluid. The four questions, read across the five windows, frame the first decisions at the bedside. Read as a set they sketch the shape of the trouble in a minute: a full tank with a weak pump points one way, an empty tank with a strained right side points another, a dry tank with a vigorous heart points a third. The five small windows add up to a picture solid enough for the first treatment to act on as the fuller study is still being arranged.
Reading them as a set
No single window tells the whole tale. The heart is one organ seen from five sides; the views are read together, each checking and filling what the others leave out. A poor parasternal window in a barrel chest is rescued by a clear subcostal one; a doubtful apex is settled by the short axis next door.
The set is the strength. A finding seen from two windows is trusted; a finding seen from one is held lightly until a second view confirms it. The discipline of running all five, even when the first looks normal, is what keeps a quiet finding in a hard-to-reach corner from slipping past. A clean first view is a reason to keep scanning, never a reason to stop, since the corner left unchecked is the one a quiet effusion or a strained right side likes to sit in.
One view hints; two views convince.
Where the windows fail
The heart does not always show itself. A barrel chest stiff with old lung disease scatters the beam, the parasternal and apical windows fading to a grey blur. Bowel gas under the ribs can swallow the subcostal view. A patient who cannot lie flat or roll left robs the apex of its best angle. Each window has a body it serves poorly, which is the deeper reason the exam carries five: when one is lost, another still reaches the heart.
The beginner’s errors are their own hazard. A marker turned the wrong way flips the heart and invents disease where none sits. A probe pressed too high or too low lands on a rib and shows nothing. A foreshortened apex shrinks the left ventricle and fakes a small, vigorous heart out of a normal one. Every one of these is undone by the same care: known landmarks, a steady marker, the patience to adjust rather than read a poor image as truth.
Learning the sweep
The five views are learned as a fixed round, drilled in order until the hand runs them without prompting. The landmarks come first, the rib spaces and the soft spot under the breastbone found by touch. Then the marker turns, one for each window, fixed by repetition. A learner who scans the same five spots on every patient, well or sick, builds the round into muscle memory, so that under the pressure of a real resuscitation the hand finds the heart while the mind is free to read it.
Drill the round on the well to read it on the sick.
The reward is a heart read in minutes by hands that are not a cardiologist’s. The focused five do not replace the full study; they bring a useful slice of it to the bedside, the trauma bay, the clinic far from any echo lab, anywhere a probe can reach a chest and a trained hand knows where to put it.
What it changed
Before the handheld probe, a question about the heart meant a wait. The patient was referred, the cart was wheeled in, the sonographer booked, the cardiologist’s reading returned in its own time, the breathless patient waiting through all of it for an answer the first minutes badly needed. The focused five put a first answer in the hands of the clinician already at the bedside, in the time it takes to lay a probe on a chest and turn it five ways.
The change was one of reach more than of depth. A full echo still says far more than five focused views ever will. The shift was in who could ask the heart a question and when, moving a slice of that power from the echo lab to the bedside, from the few to the many, from an hour’s wait to a glance. A breathless chest that once held its secret until the cart arrived now gives up the big ones to any trained hand that knows the five windows and the turns that find them.
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.