Stone in the lower pole on the handheld probe: a bright focus inside the collecting system, casting a clean shadow behind it. Credit: Wikimedia Commons (CC).
A kidney stone is found at the bedside more by what it has done than by what it is. The stone itself is small and hard, often sitting where the probe can find it; just as often, it sits where the bony pelvis hides it. The kidney behind any obstructing stone, though, gives itself away in a sign that does not hide: it swells. A handheld probe at the flank can read that swelling in seconds, the dilated calyces and the stretched pelvis lighting up as black pockets where solid grey tissue used to be. A scan that learns to read upstream first finds the stones that hide and confirms the ones that show.
Look upstream; the stone has been busy.
The kidney through the flank
The kidney reads from the side. Once it is brought into the long-axis flank window laid out on the sequence page, the bean’s three landmarks anchor the reading: a bright fatty central sinus, a paler cortex wrapping it, a thin bright capsule. Compared with the liver beside it on the right side, a healthy cortex reads a shade darker; the sinus glows brighter still. The bean is swept from pole to pole and turned across into short axis once, the sinus and the cortex weighed against the contralateral kidney as a control before any pathology is read into the picture.
The stone itself
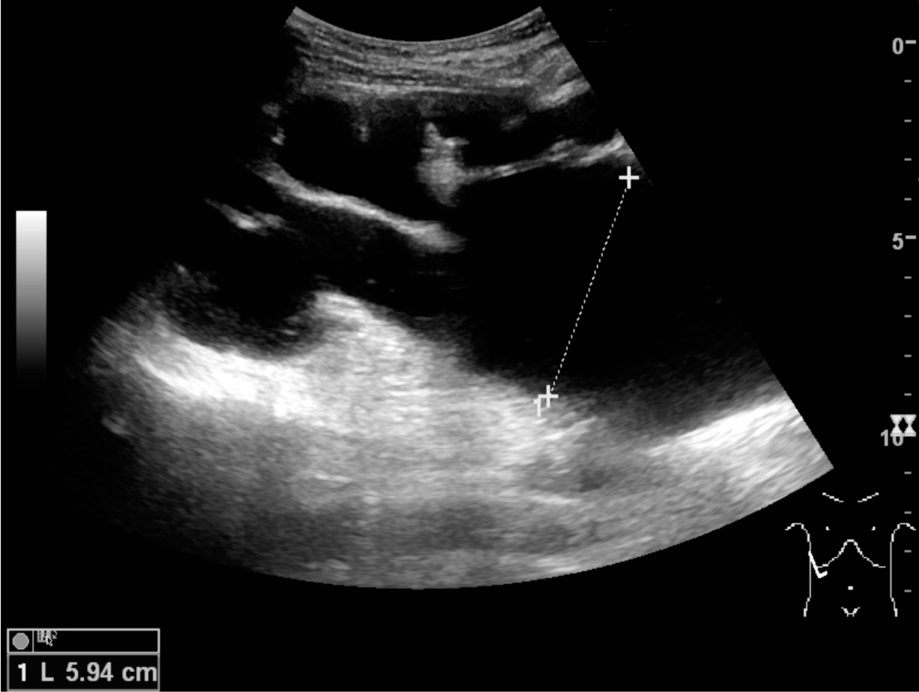
Hydronephrosis: the kidney swelling behind an obstruction, the calyces fanning out as dark pockets inside the sinus. Credit: Wikimedia Commons (CC).
A stone in the kidney is a bright echogenic focus sitting in the collecting system, where the bright sinus fat already glows; behind it falls a clean dark band of acoustic shadow that marks it apart from the fat itself. The stone need not be large to shadow; a dense calculus a few millimetres across casts a band a careful eye can spot. Position matters: a stone tucked in a calyx is easy to call when found, while a stone wedged at the pelvis or down at the ureteropelvic junction needs the probe slid across the renal sinus deliberately to be picked up. A bright focus without a clear shadow may be a stone too small to block the beam, or a wisp of vessel calcification mimicking one.
The collecting system holds the stone; the cortex does not. A bright fleck found inside the cortex itself is far more likely to be a calcified scar, an old infection nodule, or the bright pyramid tip of medullary nephrocalcinosis than an obstructing stone; nephrocalcinosis, calcium deposited within the medullary pyramids of the parenchyma, is its own disease, the bright pyramids lined up like beads inside the kidney without the collecting-system position a true urinary stone holds. The stones that block urine sit where urine flows: the calyces, the pelvis, the ureter as it leaves. The location of the bright focus carries the first half of the call before the shadow confirms the rest.
A stone sits in urine; the cortex never holds one.
The swelling that gives the stone away
A stone that obstructs the kidney leaves an upstream trail the probe sees better than the stone itself. Urine cannot pass the blockage, and the pressure backs upward into the system that carries it: the ureter dilates, then the renal pelvis stretches, then the calyces fan out into a row of dark cups inside the bright kidney sinus, the picture a sonographer calls hydronephrosis. The grading is read by eye as much as by caliper. Mild swelling shows as a black space splitting open inside the sinus, a single thin pocket of urine where the pelvis used to sit packed against the calyces. Moderate swelling rounds the calyces into communicating chambers with the cortex around them still well preserved, the bright sinus fat broken into islands floating between dark pockets. Severe swelling drowns the sinus altogether, the calyces ballooning into bulbous spaces and the cortex thinned around them, a kidney whose collecting system has taken over the parenchyma. The stone causing the obstruction may be invisible: tucked at the bony pelvic rim, hidden behind gas, or small enough, often below about three millimetres, to slip past the scan’s resolution; the kidney upstream is unmistakable. Reading the obstruction first inverts the usual hunt and pays off in the patients where the stone hides. A handheld probe set on the flank of a colicky patient finds the stone often less than half the time and finds the hydronephrosis a good deal more often, the dilated calyces telling that a stone, somewhere along the stream, has blocked the flow long enough for the kidney to swell behind it. Read upstream first: the swelling names the obstruction, and the obstruction implicates the stone.
The kidney’s tell on the stone: dark pockets fanning out where calyces have stretched upstream of the blockage.
Timing rewrites the picture. A stone that lodged in the last hour may leave a kidney still anatomically normal; the dilation needs time to build, and a colicky patient seen early can show an obstructing stone and a kidney that has yet to swell. At the other end sits long-standing partial obstruction, where the kidney has stretched gradually and the cortex around it has thinned to a rind, the dilation severe and the function in question. A single scan freezes one moment of a moving disease; a repeat hours later on the same flank, with the same probe angle, often tells the story the first look could not.
Infection inside the swollen system is the variant that turns hydronephrosis into an emergency. Pyonephrosis adds dependent echoes layering at the bottom of the dilated pelvis, a swirling debris, sometimes a fluid-fluid level where pus settles below clear urine; the patient is febrile and the kidney is obstructed and infected at once. The scan that finds debris inside a dilated system has named a kidney needing decompression in hours, not days. A clean black collecting system holds nothing to fear acutely; a cloudy one in a febrile patient changes the night, the surgeons or the radiologist called for an urgent drain.
Bilateral and unilateral patterns separate where the trouble sits. A unilateral hydronephrosis points the finger at the ureter on that side, a stone or a kink obstructing flow from one kidney alone. Bilateral dilation, especially with a large post-void residual on the bladder after the patient has tried to empty, points downstream of both ureters, at the outlet or the bladder itself, the prostate of an older man or a pelvic mass squeezing both sides; the kidneys take a back seat to a closer-to-the-floor obstruction. The first question a swollen kidney prompts is whether its mate is dry.
The kidney swells where the stone has blocked the flow above it.
Twinkle and the small bright fleck
Colour Doppler turns a doubtful stone certain. Aimed across a bright focus inside the kidney, the colour box throws back the chaotic mosaic flash of the twinkle artefact a stone is known to give, the same trick the gallstone page leans on. The kidney rewards the move in a small stone tucked at the ureteropelvic junction, in a stone packed inside a calyx that lacked a clean shadow, in a fleck the eye dismissed as sinus fat: each declares itself in colour where it stayed silent in grey. Calcified arcuate vessels along the corticomedullary line can twinkle too, the kidney’s classic mimic; a fleck inside a calyx is a stone, a fleck along the cortex is a calcification.
A twinkle picks the small stone out of the kidney’s noise.
Following the stream down
Severe, long-standing hydronephrosis: the calyces ballooned, the cortex thinned around them to a rind. Credit: Wikimedia Commons (CC).
A stone moves. Once it leaves the kidney, the probe follows the stream down, and the bladder ends the road. The proximal ureter can be picked up just past the renal pelvis on a thin patient; the middle ureter dives into the bony pelvis and hides behind sacrum and gas, beyond a handheld probe’s reach. The distal ureter reappears as it crosses behind a full bladder, and a stone wedged at the ureterovesical junction shows as a bright spot with a shadow against the bladder’s far wall. A bladder full of urine throws the window down onto that junction; an empty one closes the view, and the stone hides until the bladder refills.
Colour Doppler over the bladder catches the rhythmic squirt of urine entering from each ureter, the ureteric jets the eye can see with the colour box parked across the trigone. A patient with two intermittent jets at the trigone, the cadence varying with hydration, has both ureters open. A patient with a single jet on one side and a silent contralateral trigone has an obstructed kidney behind that silence, the jet absent or much delayed on the obstructed side. The jets are a soft sign, watched for one or two minutes, useful when the stone itself stayed hidden.
The road has limits the probe accepts. The middle ureter cannot be cleared by a handheld scan; a stone there will be inferred from a swollen kidney above and a silent jet below, and confirmed elsewhere by another study. The bedside answer is what it always answers: the kidney swells or it does not, the bladder catches what jet escapes.
Two jets at the trigone reassure; one jet alone points to the silent side.
Where the scan misleads
The scan trades its certainty for the kidney’s quirks. Parapelvic cysts, smooth fluid pockets bulging from the sinus, mimic a dilated pelvis: black, rounded, and inside the kidney’s centre. The difference is that cysts do not communicate with each other, where dilated calyces do; a long sweep that follows one black pocket into another along the renal sinus argues for hydronephrosis, where separate, isolated black ovals argue for cysts. A prominent renal pelvis without true obstruction, the so-called extrarenal pelvis, can sit large enough to look dilated when nothing is blocked at all. Comparing the two kidneys against each other answers many of these doubts: a unilateral swollen system is the suspicious one, a bilateral mild prominence with no symptoms is usually anatomy.
The reading is anchored by the company the scan keeps. A bright focus with a shadow in a calyx, a kidney that is swelling on the same side, a ureter that gives no jet at the bladder: the three together name an obstructing stone with the confidence the bedside can offer. A bright focus without a shadow, a kidney that looks dry on both sides, and two even jets at the trigone is a tube empty of stones, no matter what fleck of bright fat caught the eye. The handheld names the obstructed kidney it can see and hands the doubtful flank onward, the wider workup picking up what the scan in the room could not reach. The acute colicky workflow, the timing and the disposition of the patient in front of you, lives on the page for renal colic emergency assessment.
Read the calyces first, the shadow second; the stone confesses through the kidney it has stopped up.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.