Acute appendicitis is the inflammation of the appendix, the small blind tube that hangs off the start of the large bowel. Ultrasound finds that swollen tube at the bedside, on a probe pressed into the right lower belly. The appendix shows as a blind-ending tube wider than six millimetres, sore under the probe and refusing to flatten. The scan turns a belly pain of unclear cause into a named diagnosis in minutes. A handheld runs this look in the emergency department, the clinic, or a ward far from a scanner. The probe finds the tube, measures it, and weighs the signs of inflammation around it. A few minutes of scanning settle the question a tender belly leaves open. The appendix sits in the right iliac fossa, the corner of the belly above the hip bone on the right. The scan reaches it directly and weighs the case before any talk of an operation. A person doubled over with right-sided pain gets an answer where they lie. The workup starts here, well before a slot on the big scanner comes free.
The bedside scan spares a young belly the radiation of a CT. Appendicitis strikes often in children and young adults, the people a repeat dose of radiation harms over a lifetime. Ultrasound reaches the appendix with no dose at all. A scan-first path in a thin young patient settles many cases without a CT. The probe goes to the point of greatest pain and studies the tube right under it. A handheld brings that look to the bedside in the first minutes of the pain. The scan names a clear case and sends the doubtful ones on for more. A scan that names the disease in a young patient cuts a needless CT and its dose. A child scanned at the bedside avoids the radiation a repeated belly CT would carry. The handheld answers first and leaves the CT for the cases that earn it.
A handheld brings this scan to the patient. A clinic with no scanner of its own checks a right iliac fossa at the bedside. A rural clinician finds an inflamed appendix and arranges the transfer with the picture in hand. The diameter of the tube and the side of the pain go into the note. A saved clip of the swollen appendix travels to the surgeon. One device covers the appendix, the ovary, and the free fluid in a single sweep. The bedside scan turns a vague belly pain into a surgical plan. A pregnant patient with right-sided pain gets the same scan with no dose, the appendix often pushed up and out of its usual corner by the growing womb. The probe hunts higher in late pregnancy, where the cecum has shifted.
Hunting the appendix in the right iliac fossa
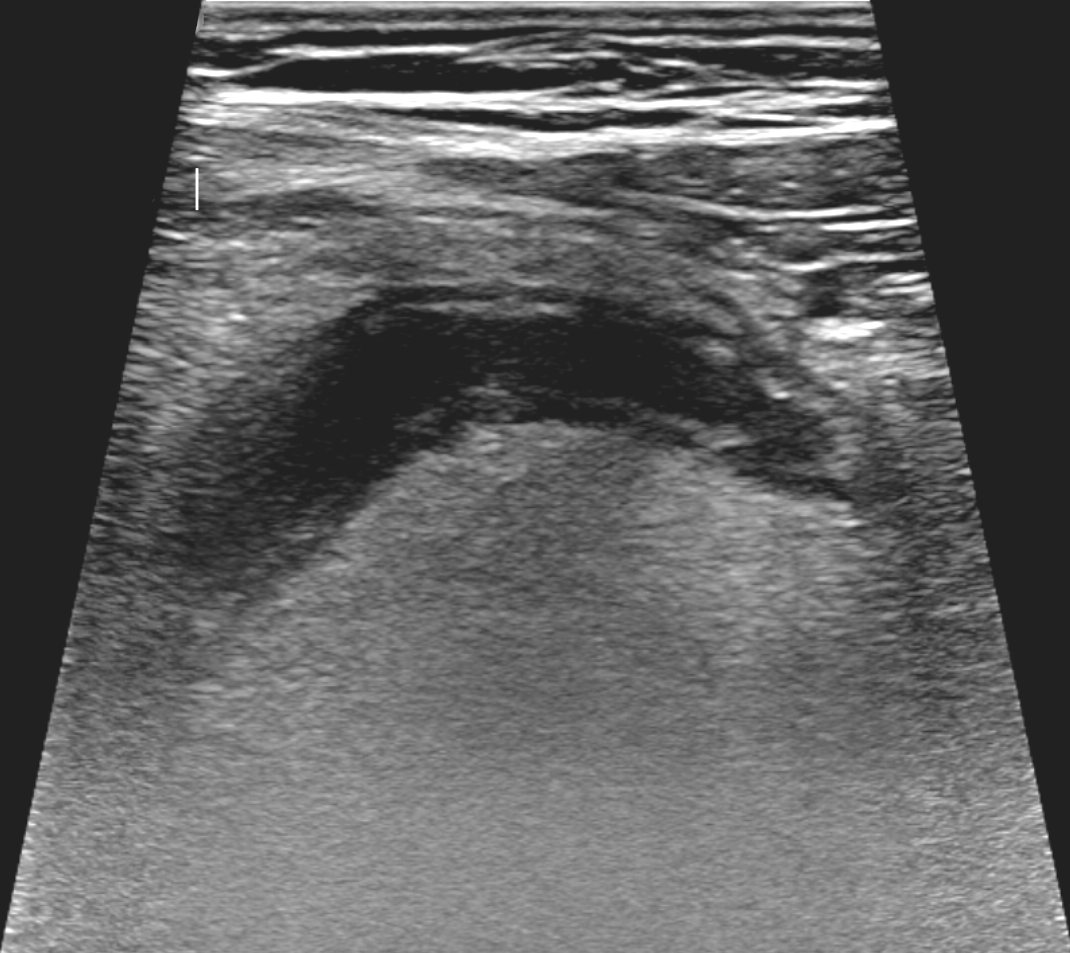
An inflamed appendix in long axis, the swollen tube running across the right lower belly. The walls stand out around the darker centre of the tube. A marker at the left edge sets the measurement. The blind-ending, non-compressible tube is the core finding of appendicitis.
Graded compression is the technique that finds the appendix. The probe presses down slowly over the point of greatest pain, easing the bowel gas aside. A steady push moves the gas and the normal loops out of the way and brings the appendix into view. The appendix holds its place under the press. A slow sweep follows the large bowel down to its end, where the appendix springs from the cecum. The right iliac fossa comes under the probe in a slow, firm sweep. A press held for a few seconds lets the gas give way. The patient points to the sorest spot. The probe starts there. The tender point under the probe marks the ground to search. The slow press is the whole trick of it. A quick jab drives the gas back and tenses the belly. A patient press over several seconds lets the gas slip aside and the bowel settle. The iliac vessels and the psoas muscle behind them give the probe its landmarks in the corner. The cecum, a gas-filled pouch, leads the way down to the appendix at its base.
The appendix is a tube closed at one end, springing from the cecum and running to a blind tip. No peristalsis travels along it. A normal small bowel loop squeezes and relaxes under the probe and flattens to a press. The appendix does neither. The blind end, traced to its tip, proves the tube is the appendix. The probe follows the tube to that closed end to be sure. A round, fixed tube that will not flatten is the one to measure. The trace from the cecum to the blind tip rules out a loop of gut passing through. The cecum is the signpost. A gas-filled cecum, found first, leads down to the point where the appendix buds off its tip. A tube that springs from the cecum and ends blind is the appendix and nothing else.
The appendix hides in more than one spot. A retrocecal appendix tucks behind the cecum, out of the easy line of the probe. A turn of the patient onto the left side rolls the cecum up and brings a hidden appendix forward. The appendix can dip into the pelvis or point up toward the liver. A wider search opens when the tube does not sit where it should. A posterior approach through the flank reaches an appendix tucked behind the bowel. Patience and a moving probe find a tube that the first sweep missed. An appendix low in the pelvis can sit behind the bladder, reached through a full bladder as a window. A long appendix can reach up under the liver and ape a gallbladder pain. The search runs wide when the corner comes up empty.
The patient leads the probe to the appendix. The point of greatest pain under the probe, the sonographic McBurney sign, sits right over the inflamed tube in many cases. A press where the finger points brings the tube beneath into view. A tube found right under the sorest spot carries weight on its own. The pain and the picture line up over the same point. The bedside scan weighs the tenderness and the tube together. A pain that holds to one fixed spot points to a local trouble like an inflamed appendix. Pain felt across the whole belly speaks for something past one organ. The sore point under the finger leads the scan straight to the tube.
The signs of an inflamed appendix
A long-axis scan of the right lower belly, the SAG RLQ label at the lower left. The red arrow marks the appendix; the calipers measure it at about twelve millimetres across, twice the six-millimetre line. A tube this wide, sore and refusing to flatten, is an inflamed appendix.
The width of the appendix sets the diagnosis. A normal appendix measures under six millimetres across, outer wall to outer wall. A tube over six millimetres in the right setting is an inflamed appendix. The calipers cross the swollen tube at its widest in the short axis. The measurement runs from the outer edge of one wall to the outer edge of the other. A tube at seven or eight millimetres with pain over it makes a confident call. The diameter, measured at the bedside, is the number the surgeon plans against. A borderline tube near six millimetres earns a closer look at the other signs. The single widest measure across the tube carries the weight. Graded compression ultrasound names an inflamed appendix in about eighty-seven of a hundred people who have one. A tube over six millimetres, still sore under the probe, carries the diagnosis at the bedside. The six-millimetre line is a guide, with a grey zone right around it. A tube at exactly six millimetres sits right on the line, judged on the signs around it. A larger tube makes a surer call. The measurement carries its full weight when the tube is sore, round, and fixed at the same point.
The inflamed appendix refuses to flatten under the probe. The swollen tube holds its round shape against a press, too tense with inflammation to give way. The non-compressible tube is the heart of the diagnosis. The press goes on gently, in grades, never a hard jab on a tense belly. The press eases on enough to test the tube and stops short of pain. A tube that springs back round after each press is the non-compressible appendix. The finding holds up along the length of the tube, tested at several points. A cross-section shows a target: a round tube with layered walls, a bright centre ringed by a dark muscle layer. The target sign names the appendix in cross-section the way the blind tube names it along its length. The bright centre of the target is the lining and the trapped contents. The dark ring around it is the swollen muscle wall. The long view shows the blind-ending tube. The short view shows the target. Two views of the same tube, across and along, lock in the call. An appendix filled with fluid widens into a dark tube along its length, the trapped secretions stretching it behind a blockage at its mouth. The clean layers of an early tube blur when the disease climbs. A wall that has lost its layers warns of a tube under threat. The probe studies the wall along the whole tube for the state of the disease. Colour and spectral Doppler sharpen a borderline tube, the inflamed wall lighting up with flow on the colour box. A borderline appendix with a hot wall on Doppler leans toward the disease. The layered wall, the target in cross-section, and the blind tip in long axis build one picture from three angles. A gut-signature wall, its bright lining and dark muscle in clean rings, marks an early tube. The tube, tested at several points along its length, holds its swelling through the run.
The signs stack into one picture: a blind tube over six millimetres, round, non-compressible, and sore under the probe. A diameter, a shape, and a tenderness together name appendicitis with little room for doubt. Each sign on its own leaves a question. Stacked together, the three settle the call. A clip of the swollen tube and its measure travels with the referral. The whole picture costs nothing and carries no dose. The three core signs together carry more weight than any single one. A wide tube alone can be a normal variant. A non-compressible tube alone can be a stiff loop. A tender spot alone can be many things. The three stacked on the same tube name appendicitis.
Colour Doppler adds the heat of inflammation. The wall of an inflamed appendix lights up with flow, a ring of colour around the tube. The hyperaemia marks a tube alive with inflammation. A faint or absent flow in a swollen tube can warn of a wall losing its blood supply. The colour box held over the tube shows the state of the wall. A bright ring of flow backs the diagnosis on a swollen, sore tube. A ring of fire around the tube on colour Doppler is the classic mark of a hot appendix. The flow fades when a wall dies, a late, ominous turn. The colour box adds its weight to the grey-scale picture.
The fat around the appendix turns bright with inflammation. Inflamed fat glows whiter than the fat elsewhere, a halo of brightness around the sore tube. The bright fat points the probe toward an appendix the gas hides. A pocket of free fluid can sit beside the inflamed tube. Dark fluid around the appendix backs the picture of inflammation. The bright fat and the fluid together raise the worry even before the tube comes into clear view. The probe studies the corner of the belly for the signs around the tube. Inflamed fat is a quiet, telling sign, the brightness around a tube the eye learns to trust. A mat of bright fat in the right corner often marks the appendix before the tube itself comes clear. The fluid, the fat, and the heat on Doppler together build the case.
The appendicolith and what it warns of
An appendicolith is a hard stone lodged in the appendix. The stone shows as a bright dot with a dark shadow behind it, sitting in the tube or at its mouth. A stone at the mouth blocks the tube and drives the inflammation behind it. The appendicolith raises the chance of a tube that will burst. A stone seen in a swollen appendix moves the case toward an earlier operation. The shadow behind the bright dot marks the stone out from a fold or a bubble. The probe hunts the stone along the tube and at the cecal end. A stone in the appendix shows up in a fair share of inflamed tubes and warns of trouble ahead. The blocked tube behind a stone swells faster and bursts sooner. A stone seen on the scan tips a borderline case toward the operating room.
The blockage at the mouth sets the disease in motion. A stone, a swollen lymph node, or a kink shuts the tube at its base. The trapped secretions stretch the tube behind the block and feed the bacteria inside. The pressure climbs until the wall gives way. A wide, fluid-filled tube with a stone at its mouth tells that whole story in one picture. The scan catches the cause and the effect together. A free flow of fluid through the belly, beyond the corner, warns of a tube that has burst and spilled. A spreading collection points the surgeon toward an abscess to drain. The scan grades the trouble from a tight tube to a leak loose in the belly.
Appendicitis on ultrasound: the numbers
What is measured
Value
What it points to
Appendix diameter
over 6 mm
inflamed appendix
Appendix diameter
under 6 mm
normal appendix
Tube under compression
will not flatten
inflammation
Appendicolith
bright dot with shadow
higher risk of bursting
Ultrasound sensitivity
about 87%
strong when the tube is seen
Ultrasound specificity
about 90%
few false alarms
When the scan cannot find it
The appendix does not always come into view. Gas, a deep retrocecal tube, or a large belly can hide it. A scan that fails to find the appendix does not clear the diagnosis. The secondary signs carry the case when the tube stays hidden. Bright inflamed fat, a pocket of fluid, or a thick-walled cecum in the right setting all point to an appendix the probe cannot reach. A convincing story with secondary signs and no visible appendix still earns a careful watch or more imaging. The failure to see the tube is not the same as a normal appendix. Bowel gas is the usual reason the tube hides. A heavy belly, a deep retrocecal tube, or a perforated appendix that has decompressed can each keep it out of view. A perforated tube can shrink back and grow hard to find, the case that needs the surgeon without delay. A scan empty of the tube, with secondary signs all around, still moves the case forward.
The secondary signs speak when the appendix hides. A halo of bright fat in the right iliac fossa points to inflammation under it. A pocket of free fluid in the corner backs the picture. A loop of bowel near the tube can stop moving, stunned by the inflammation beside it. A small lymph node or two can swell near the sore tube. The signs together raise the worry even with the appendix out of view. The scan gathers them up before calling itself clear. A soft, rounded reactive lymph node can swell beside the sore tube. A short length of bowel near the appendix can fall still, its movement stunned by the inflammation. The probe weighs these quiet signs together when the tube plays hard to find.
Other troubles can mimic the pain of appendicitis. An inflamed ovary or a twisted one gives a pain on the same side. A swollen lymph node in a child can look like an appendix, a milder cause with no danger in it. The probe checks the ovary in a woman and the bowel around the tube before settling on the appendix. A right iliac fossa pain earns a look at more than the appendix alone. The scan rules the other causes in or out alongside the tube. Mesenteric adenitis fills the corner with swollen nodes and a normal appendix, a milder trouble that settles on its own. A terminal ileitis thickens the last loop of small bowel and can mimic the pain. An ovarian cyst or a twisted ovary on the right gives a pain on the same side, caught by a sweep of the pelvis. A ureteric stone high in its course can throw a pain to the same corner.
A clean look at a normal appendix carries its own weight. A thin tube under six millimetres that flattens to a press is a normal appendix. A normal appendix found and measured argues against the diagnosis. The probe that finds a soft, thin tube can calm a worried belly. A normal scan with an easing pain sends a person home with a plan to return. The bedside look settles the calm cases as well as the sick ones.
When the disease has gone further
A perforated appendix can collapse and leak. A pocket of fluid with bright debris beside a broken tube marks an abscess.
One probe at the bedside
A borderline appendix earns a second look. A tube near six millimetres with little around it sits in doubt. A repeat scan a few hours on can settle it. On the second look, a tube swollen past six millimetres confirms the disease. A tube that stays thin, flattening to a press, turns the search elsewhere. The handheld follows a doubtful tube over hours with no dose at all. The bedside scan watches a borderline case in place of a rush to the operation. The pain and the tube, checked again, sort the sick from the settling. A doubtful tube watched over a morning declares itself. A swelling that grows confirms the disease. A swelling that fades sends the worry off. The repeat scan spares a needless operation on a tube that settles.
The handheld names the clear cases and hands the hard ones on. A CT or an MRI maps a doubtful belly when the scan leaves a question. A pregnant patient or a child gets the ultrasound first, with no radiation at all. The scan answers the first question in minutes and points the way. A clinic that owns no scanner works up a right iliac fossa pain at the bedside. A nurse, a junior doctor, or a rural clinician each learn the appendix look. The probe that found the tube sends the patient to the surgeon with the measure in hand. An MRI maps a doubtful belly in a pregnant patient with no radiation at all. A CT settles a heavy or unclear belly in an adult where the tube stays hidden. The bedside scan opens the path. The cross-sectional scan finishes the map when the question stands.
One probe holds the whole right-iliac-fossa look at the bedside. The appendix found, measured, and judged, the bedside scan points the way in minutes. The scan repeats over hours without a bill or a dose. A swollen tube watched over a morning gives up its trend. The skill takes a handful of scans to build and serves for a career. The same probe that found the inflamed appendix sends the patient to the room that can fix it.
Common questions
Can ultrasound diagnose appendicitis?
Ultrasound finds an inflamed appendix as a blind-ending tube wider than six millimetres, round, non-compressible, and sore under the probe. Graded compression eases the bowel gas aside to bring the tube into view. The scan is strong when it finds the tube. A clear inflamed appendix names the diagnosis at the bedside. A scan that cannot find the tube does not clear the diagnosis on its own.
How big is an inflamed appendix on ultrasound?
A normal appendix measures under six millimetres across, outer wall to outer wall. A tube over six millimetres with pain over it points to appendicitis. A tube at seven or eight millimetres makes a confident call. A borderline tube near six millimetres earns a look at the other signs and a repeat scan.
What is graded compression?
Graded compression is a slow, steady press over the right lower belly that eases the bowel gas aside. The soft normal gut flattens and slips away under the press. The inflamed appendix stays round and will not compress, the finding that names it. The technique brings a hidden tube into view and shows whether it gives way.
Why does appendicitis get scanned before a CT?
Appendicitis strikes often in children and young adults, the patients who carry the greatest lifetime cost from radiation. Ultrasound reaches the appendix at the bedside with no dose at all. A clear scan names the disease and sends the patient to the surgeon. A doubtful belly goes on for a CT or an MRI to map the cause.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.