Acute cholecystitis is the inflammation of the gallbladder, the small sac under the liver that stores bile. Ultrasound finds that angry gallbladder at the bedside, on a probe pressed under the right ribs. The scan shows a stone stuck in the neck, a thick wall, and a sac sore right under the probe. The three together name the disease in minutes. A handheld runs this look in the emergency department, the clinic, or a ward far from a scanner. The probe finds the gallbladder, hunts the stones, and tests the sore spot over it. A few minutes of scanning settle the cause of a pain under the right ribs. The gallbladder sits under the edge of the liver, on the right, below the ribs. The scan reaches it directly and weighs the case before any talk of an operation. A person gripping the right upper belly gets an answer where they lie. The workup starts here, well before a slot on the big scanner comes free.
Ultrasound is the first test for a pain under the right ribs. The scan finds the stones that start the trouble and the wall that marks the inflammation. The handheld answers at the bedside in the first minutes of the pain. A stone seen stuck in the neck of a sore, thick-walled sac names cholecystitis on the spot. The probe goes to the point under the ribs where the pain bites and tests the gallbladder right there. The bedside look spares a wait for a scanner in another room. A person too sore to lie flat gets the scan where they sit. A scan that names a stone-blocked, inflamed sac sends the patient toward the operation without delay. A handheld carries that answer to the trolley, the clinic, or the ward. The bedside look opens the path that a scanner in another room would only slow.
A handheld brings this scan to the patient. A clinic that owns no scanner checks a gallbladder at the bedside. A rural clinician finds an inflamed sac and arranges the transfer with the picture in hand. The thickness of the wall and the stone at the neck go into the note. A saved clip of the sore gallbladder travels to the surgeon. One device covers the gallbladder, the bile duct, and the liver in a single sweep. The bedside scan turns a right-sided belly pain into a surgical plan. A picture of the stone and the thick wall, sent ahead, warns the surgeon before the patient arrives. A clinic far from a hospital names the disease and starts the referral that gives a chance.
The pain of a hot gallbladder sits under the right ribs and bores through to the back or the shoulder blade. A pain that came after a fatty meal and would not settle points to the gallbladder. A fever and a sore right upper belly raise the worry of an inflamed sac. The scan puts a picture to that pain in minutes. A vomiting patient gripping the right ribs gets the gallbladder scanned first. A pain that grips for hours, past the usual hour of a simple colic, leans toward an inflamed sac. The fever, the sickness, and the sore right ribs together raise the case from a passing stone to cholecystitis. The scan sorts the two at the bedside.
Finding the gallbladder under the ribs
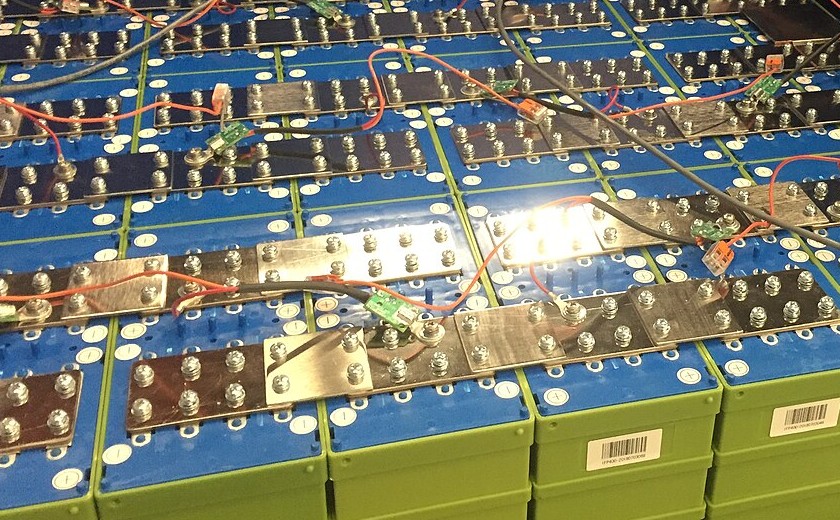
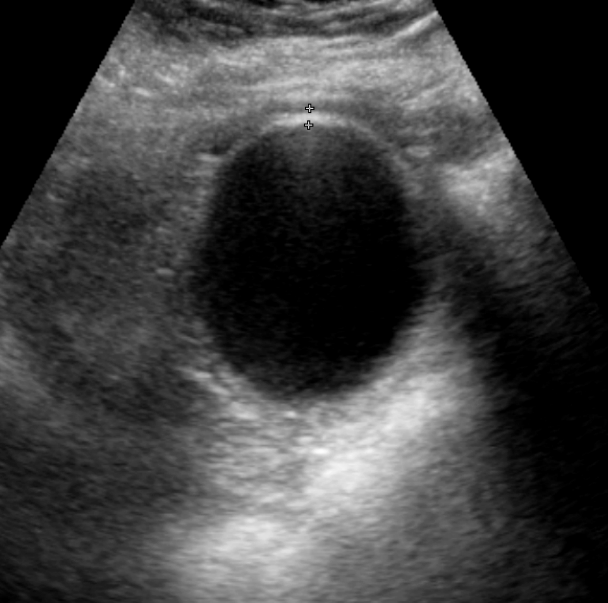
A gallbladder in cross section, the calipers at the top measuring the wall at about three and a half millimetres, just past the three-millimetre line. The dark oval is the bile-filled sac. A wall this thick, with stones and a sore spot under the probe, points to early cholecystitis.
The probe slides under the right ribs and angles up toward the liver. The gallbladder shows as a dark sac hanging off the underside of the liver. A deep breath drops the liver and the gallbladder down past the ribs into view. A rock of the probe between the ribs clears the bone and the bowel gas. The gallbladder runs from its rounded base to its narrow neck, where it meets the bile duct. A sweep along the whole sac, from base to neck, catches a stone at any point. The patient breathes in and holds while the probe finds the sac. The neck of the gallbladder hides a stone that the base would miss, swept on every scan. A roll onto the left side shifts a stone and shows whether it moves. The sac comes into a long view and a short view to measure it true. The main fissure of the liver runs as a bright line from the portal vein to the neck of the gallbladder, the landmark that finds the sac when the bowel gas crowds it. A subcostal sweep catches the gallbladder under the ribs; an intercostal view reaches one tucked high. The fasting gallbladder fills with bile and shows clearly. A sac scanned soon after a meal collapses and hides, the reason the scan waits for an empty stomach. A contracted sac after a meal can fake a thick wall, the folded empty walls stacked into a false thickness. A scan on a fasting belly clears that trap.
A gallstone shows as a bright curve with a dark shadow behind it. The shadow is the proof of a hard stone, marked out from a fold or a polyp. Ultrasound finds gallstones in more than nine of ten people who carry them, the surest part of the scan. A free stone rolls to the low side of the sac when the patient turns. The stone that stays put at the neck is the dangerous one, wedged where it blocks the sac. A sweep of the sac catches every stone, with the neck watched for one wedged there. A sac packed with stones can hide its wall behind a band of bright echoes and a shadow. The bright wall, the stones, and the shadow together mark a gallbladder full of stones. The size of a stone runs from a fleck of grit to one that fills the neck. A tiny stone can hide in the folds, brought out by a roll of the patient and a careful sweep. A polyp on the wall holds still as the patient turns and throws no shadow, the mark that sets it apart from a stone.
The probe doubles as the examining hand. A press of the probe straight onto the gallbladder finds the sore spot the disease marks. The patient catches a breath when the probe meets an inflamed sac. The tenderness lands right on the gallbladder itself, sharp at that one point. The probe sees the sac and tests it sore in the same move. The pain and the picture meet over the same point. A sore spot that sits right on the gallbladder, true to the sac and nowhere else, is the sign to trust. A lift of the probe and a second press make sure the tenderness tracks the sac.
The signs of an angry gallbladder
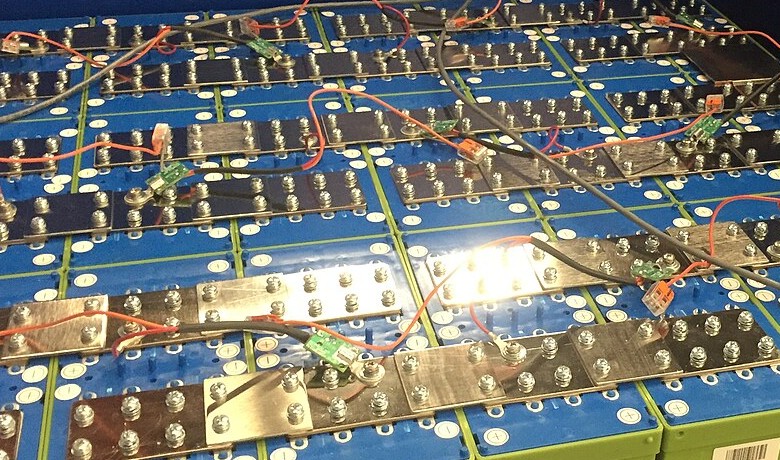
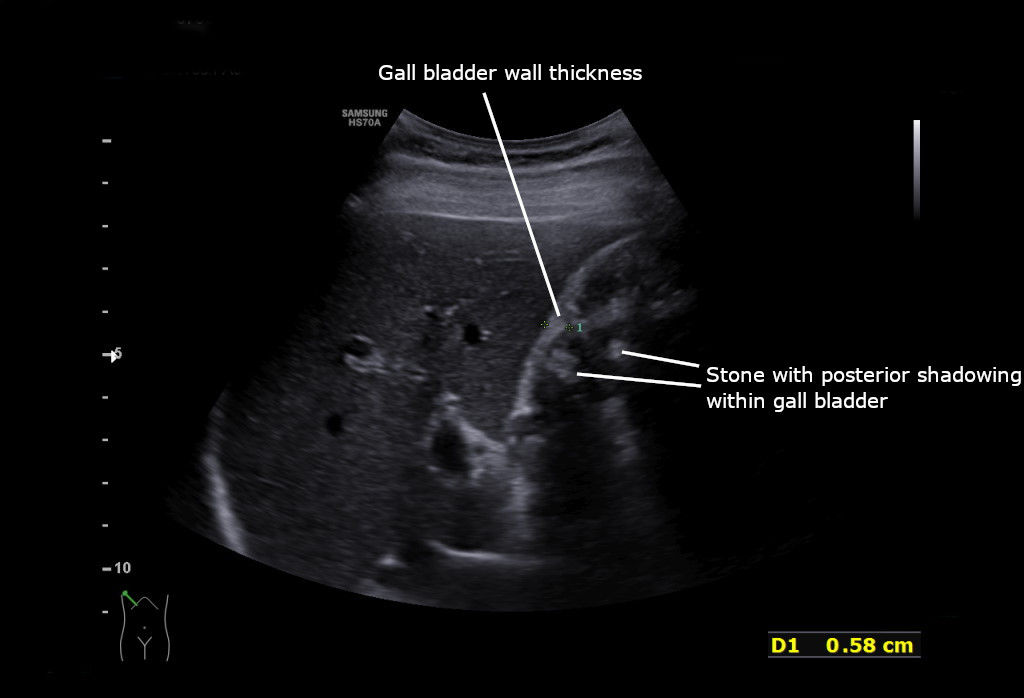
Acute cholecystitis on ultrasound. The label and calipers mark the gallbladder wall, measured at 0.58 centimetres, nearly twice the three-millimetre line. The lower label marks a stone casting a dark shadow behind it inside the sac. A thick wall and a stone together name the diagnosis.
The wall of the gallbladder thickens with inflammation. A normal wall measures under three millimetres. A wall over three millimetres in a sore sac with stones points to cholecystitis. The calipers cross the front wall of the sac, where the measure is cleanest. A wall at four or five millimetres with pain over it makes a confident call. The thick wall can layer into stripes of light and dark, the oedema spreading through it. The measurement, taken at the bedside, sets a number on the inflammation. A thin wall under three millimetres argues against an angry gallbladder. The single clearest measure of the front wall carries the weight. The wall thickens in a smooth line early on. It breaks into uneven stripes when the disease worsens. A focal bulge in the wall can hide a stone burrowing in or a growth, marked for a closer look. A wall thick all the way round speaks for inflammation through the whole sac.
The sonographic Murphy sign adds the fourth thread to the picture. The tenderness lands right on the sac under the probe, the sign of the gallbladder as the source of the pain. A positive sign over a stone-filled, thick-walled sac builds a strong case for cholecystitis. The sign fades in a gallbladder whose wall has died, a quiet sac a dangerous turn. The three core findings stack into the diagnosis: a stone, a thick wall, and a sore sac under the probe. A stone at the neck, a wall over three millimetres, and a positive Murphy sign together name the disease with little doubt. Each finding alone leaves a question. A stone alone is common and often quiet. A thick wall alone has many causes. A sore spot alone can be many things. The three on the same gallbladder settle the call. A rim of dark fluid tracking around the sac, the pericholecystic fluid, marks inflammation spilling past the wall. The fluid around the gallbladder warns of a sac under real strain. The probe tests the Murphy sign last, after the sac and the stones come clear, so a guarded belly does not hide the rest. The stone, the wall, the sign, and the fluid build one picture from four angles. A clip of the stone and the thick wall travels with the referral, the whole study in a few minutes at no dose. The probe presses gently for the Murphy sign, easing on, never jabbing, so the test holds true. A sign gone missing does not clear the disease, since a dying wall loses its feeling. The combination carries the weight, far past any lone sign, the way the surgeon weighs the scan. The fluid, the wall, and the stone come together, never one at a time, the way a hot gallbladder shows itself.
A hot gallbladder swells under the block. A sac stretched past four centimetres across, taut under the pressure, points to a gallbladder under strain. The blocked sac fills with bile and cannot empty, swelling against its wall. A distended sac with a stone at the neck tells the story of the block. The probe measures the sac across its width for the size of the strain. A sac that has ballooned past its normal size, tense under the block, marks the pressure of a blocked outlet. The wall stretches thin over a tense sac early, then thickens once the inflammation builds. The size of the sac, set against its normal slim shape, shows the weight of the block.
Colour Doppler shows the heat in the wall. An inflamed gallbladder wall lights up with flow, the vessels engorged with the inflammation. A hot wall on Doppler backs a thick-walled sac with pain over it. The flow climbs in early inflammation. It fades when a wall dies. The colour box adds its weight to the grey-scale picture. A wall with no flow at all, dark on Doppler in a sick sac, can warn of a wall that has died. The colour box shows the life left in the wall.
A gallbladder packed with stones can shrink to a thin line. The near wall, a bright echo, and a broad shadow line up as the wall-echo-shadow sign, a sac full of stones with no bile left to see. A contracted, stone-filled gallbladder gives that triple line under the ribs. The probe takes the wall-echo-shadow as a gallbladder full of stones, set apart from an empty loop of bowel. A sac that will not fill or move marks an old, scarred gallbladder. The bedside scan tells a packed sac from a normal one by that bright line and its shadow. A comet-tail behind a bright fleck in the wall marks crystals lodged in it, a sign of a different gallbladder trouble. The wall-echo-shadow holds when no bile is left to fill the sac, the way to name a gallbladder packed solid with stones.
Acute cholecystitis on ultrasound: the numbers
What is measured
Value
What it points to
Gallbladder wall
over 3 mm
inflamed gallbladder
Gallbladder wall
under 3 mm
argues against it
Gallbladder width
over 4 cm
a sac under pressure
Bile duct
over 6 to 7 mm
a backed-up drain
Ultrasound for gallstones
about 95% sensitive
strong for stones
Ultrasound for cholecystitis
sens ~71%, spec ~85%
strong with the cluster
When the wall lies
A thick wall is not always cholecystitis. A failing heart, a low blood protein, or a sick liver can thicken the wall with no stone in sight.
The stone at the neck and the bile that backs up
A stone wedged in the neck is the engine of the disease. The blocked neck traps the bile and lets the pressure climb behind it. A stone fixed at the neck, held there as the patient turns, marks the block that starts cholecystitis. The trapped bile feeds the inflammation and the wall thickens against it. A careful sweep hunts the neck on every scan for a stone wedged out of the easy view. A stone that hides in the neck behind the bowel gas asks for a roll of the patient to bring it out. The neck holds the stone that the base would never show. A big stone jammed in the neck can press on the bile duct beside it and back up the bile, a trouble in itself. The probe checks the duct above a neck stone for a squeeze from outside. A stone at the neck earns a look at the duct it sits against.
The bile duct runs beside the gallbladder and tells its own story. A duct over six or seven millimetres across has backed up behind a block. A stone that has slipped from the gallbladder into the duct dams the bile and yellows the patient. A sweep follows the duct from the liver toward the gut for a stone or a swell. A wide duct with a sore gallbladder points past a simple stone to a blocked drain. The scan checks the duct on every right-sided pain that turns the skin yellow. A duct that has widened with age can measure large with no stone behind it, judged against the patient’s years. A stone in the duct can slip through and leave a wide duct as its only trace. The probe times its check of the duct to the colour of the skin and the level of the bile salts.
The variants that kill
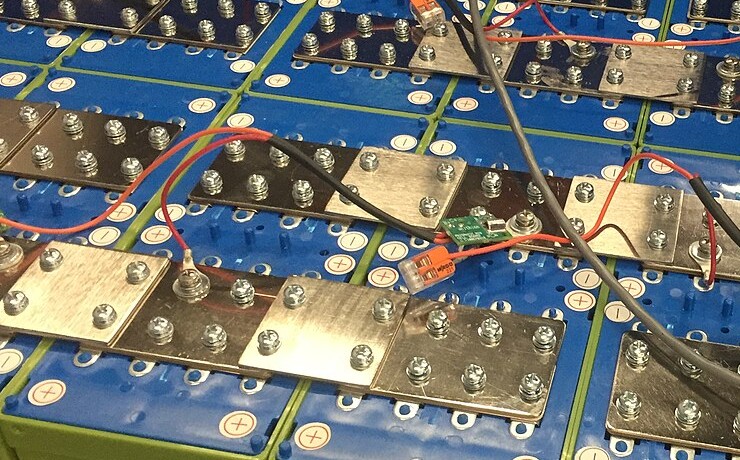
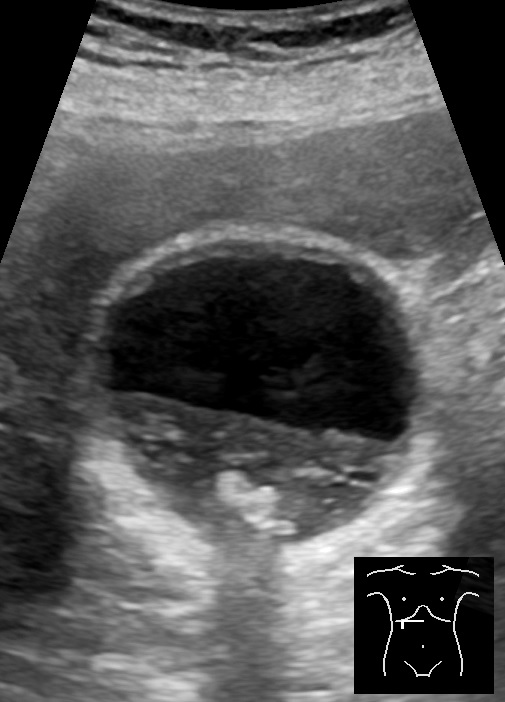
A gallbladder filled with sludge and stones. The bile settles into layers, the heavier sludge sinking to a level across the sac. Bright stones gather at the bottom and cast shadows below. The small body icon at the lower right marks the probe position.
A gallbladder wall can die when the pressure chokes its blood. A gangrenous gallbladder shows a wall broken into uneven stripes, with membranes peeling into the bile inside. The sore spot can fade when the nerves in a dying wall go quiet, a falling Murphy sign over a worsening sac. A wall that has lost its smooth line, shed membranes into the bile, warns of gangrene. The scan catches the danger that the easing pain would hide. A patient whose pain drops as the sac turns gangrenous needs the surgeon faster, with no comfort taken from the easing pain. Membranes peeling off the wall float in the bile as fine bright strands, a sign of a wall coming apart. The smooth inner line of a healthy wall gives way to a ragged, broken edge. The scan takes the ragged wall and the floating strands as a gallbladder past saving by drainage alone.
Gas in the wall marks a gallbladder rotting from within. An emphysematous gallbladder shows bright flecks in its wall that ring and shadow like gas. The bright gas rises to the top of the sac and shifts as the patient turns. A gallbladder wall full of gas points to a severe infection that races ahead. The scan names this emergency at the bedside and sends it straight to the surgeon. A diabetic patient with a hot belly and gas in the wall has no hours to lose. The gas in the wall can ring like a string of bright beads, the champagne sign of a sac full of gas. A dirty shadow trails the gas, murkier than the clean shadow of a stone.
A gallbladder can turn dangerous with no stone at all. Acalculous cholecystitis strikes a sick patient in intensive care, the sac inflamed without a stone to blame. A thick wall, a tense sac, and pericholecystic fluid name it when no stone shows. A look at the wall and the fluid carries the case in a patient too sick to point to the pain. A sore, swollen gallbladder with no stone in a critically ill patient earns a close look. The scan finds the inflamed sac that the missing stone would let slip. A patient on a ventilator, fed through a vein, can grow an inflamed sac with no stone and no way to complain of pain. The scan stands in for the history a sedated patient cannot give. A thick wall and fluid around the sac in a patient going downhill earn a drain or an operation.
An inflamed gallbladder can burst. A wall broken open spills bile and pus into a pocket beside the sac. A collection of fluid around a torn gallbladder marks a perforation that needs the surgeon now. A sweep around the sac hunts for a leak gathering beside it. A gallbladder that has burst hides its danger behind a belly that may ease for an hour. The scan grades the trouble from a hot wall to a sac that has given way. A walled-off leak can form an abscess, found as a pocket of murky fluid beside the sac. A free leak spills into the wider belly and turns a local trouble into a spreading one. A contained pocket or bile loose in the belly sets how fast the surgeon must move.
The probe on the tender gallbladder
One probe holds the whole gallbladder look at the bedside. The stone found, the wall measured, the sore spot tested, the bedside scan points the way in minutes. A clear scan of a stone-filled, thick-walled, sore sac sends the patient to the surgeon. A doubtful case goes on for a HIDA scan or a CT to settle the question. A pregnant patient or a sick child gets the ultrasound first, with no radiation at all. A nurse, a junior doctor, or a rural clinician each learn the gallbladder look. The probe that found the inflamed sac sends the patient to the room that can take it out. A patient too sick for an operation can have a tube placed through the skin to drain the inflamed sac, a bridge until they mend. The scan guides that drain and watches the sac settle after. The handheld follows a drained gallbladder over the days it takes to cool.
The bedside scan proves itself in a pain under the right ribs. The gallbladder comes up faster than any other test, the stones and the wall named on the spot. The scan repeats over hours at no charge, with no radiation. A sore sac watched over a day gives up its trend. The skill takes a handful of scans to build and serves for a career. The same probe that found the angry gallbladder sends the patient to the surgeon with the picture in hand. A sore, thick-walled gallbladder scanned today comes back to the same probe tomorrow to track its course. A sac that cools on treatment, its wall thinning and its pain easing, shows the cure taking hold. The same skill serves a nurse, a junior doctor, and a surgeon alike.
Common questions
Can ultrasound diagnose acute cholecystitis?
Ultrasound names acute cholecystitis from a cluster of signs: a stone stuck at the neck, a wall over three millimetres, a tender spot under the probe, and dark fluid around the sac. Ultrasound finds gallstones in more than nine of ten people who carry them. No single sign carries the diagnosis. The findings stacked together on one gallbladder make the call at the bedside.
What is the sonographic Murphy sign?
The sonographic Murphy sign is tenderness felt right under the probe as it presses on the gallbladder. The patient catches a breath when the probe meets an inflamed sac. The tenderness lands on the gallbladder itself, sharp at that one point. A positive sign over a stone-filled, thick-walled sac builds a strong case for cholecystitis.
How thick is the gallbladder wall in cholecystitis?
A normal gallbladder wall measures under three millimetres. A wall over three millimetres in a sore sac with stones points to cholecystitis. A wall at four or five millimetres with pain over it makes a confident call. A thick wall has other causes too, so it carries weight only alongside a stone and a tender spot.
What does ultrasound show in a dangerous gallbladder?
A gangrenous gallbladder shows a wall broken into uneven stripes with membranes peeling into the bile. An emphysematous gallbladder shows bright gas in the wall that rings and shadows. Acalculous cholecystitis inflames the sac with no stone, often in a critically ill patient. Each of these turns names an emergency that goes to the surgeon at once.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.