
























Veterinary Echocardiography Handheld for Dogs and Cats vTTE
A veterinary heart scan reads the beating heart through the chest wall, the chambers filling and emptying live on the screen. The handheld version is a focused scan, answering the questions that cannot wait in the consult room: whether the heart is pumping, whether its chambers have stretched, whether fluid has gathered around it. Grading the disease in full is the cardiologist’s work.
Why a heart scan, and when
The heart scan follows a real finding. It is never run on a hunch. A murmur picked up on the stethoscope is the commonest trigger, a whoosh over the heart where the blood should run quiet. The scan reads what lies behind that sound, the leak or the strain the ear cannot name.
Other animals arrive with the trouble already showing. A dog coughing through the night, a cat breathing fast at rest, an animal that fainted and came round on the floor: each carries a question the heart scan can settle. The scan reads whether the heart is the cause or an innocent bystander.
Some scans are run before any sign at all. A breed at risk of heart disease is screened young, the heart read before a murmur or a symptom shows, so an owner and a vet can plan around what is coming. A clean heart on the screen is an answer in itself. A heart scan earns its place the moment a sign points at the chest. A cough that will not settle, a faint on a walk, a belly filling with fluid, a murmur heard for the first time: each sends the probe to the heart to read what lies behind the sign.
The questions a focused scan answers
The focused heart scan is built around a few set questions. A vet reaches for it when an animal comes in coughing, fainting, breathing hard, or found to have a murmur. The scan looks for the handful of answers that change what happens that same day. A focused scan does not try to do everything. It leaves the fine grading, the valve-by-valve flow study, and the search for the rarer defects to the full echo. What it does, it does fast, and it does at the bedside where the answer is needed.
The first answer is whether the heart pumps. The eye watches the walls close in on the chamber, one beat at a time. A muscle in failure barely stirs, its walls drifting where they should drive in hard. That weak motion reads straight off the moving picture, well before any measurement is taken.
The second answer is the size of the chambers. A chamber stretched wide carries a heart under strain. The third answer is fluid, a dark rim gathering around the heart, the find that turns a routine scan into an emergency. These three together steer the next hour of care. A scan that reads all three as normal is an answer in its own right, turning a breathless animal away from the heart and toward the lungs or the airways as the cause.
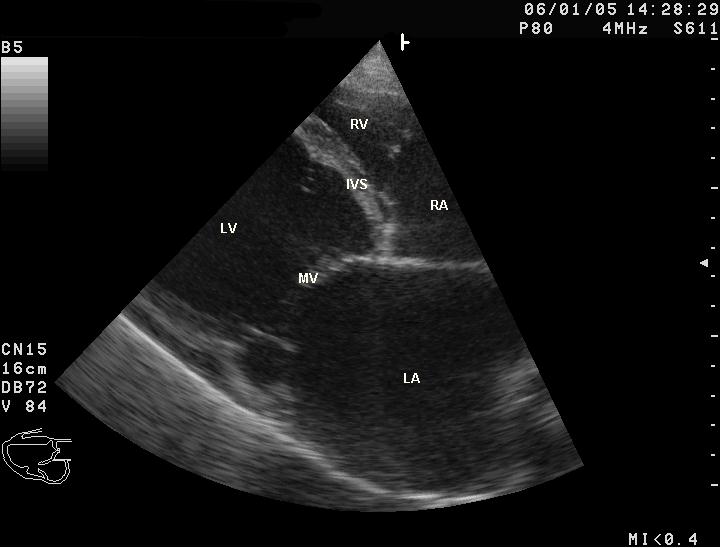
The heart hides behind the ribs and the air-filled lung, so the sound reaches it through narrow gaps. The main window sits low on the right chest wall, behind the elbow, where the heart leans against the body wall and the lung pulls clear. From there the probe looks straight into the chambers. The probe itself is a small one, a phased or microconvex head that fits between the ribs and fans a wide beam from a narrow point of contact.
A turn of the probe opens two views from that one spot. The long view runs the heart head to tail, the chambers stacked in a row. A quarter turn gives the short view, a round slice that cuts across the heart like a loaf. The left chest gives a third window for the flow studies a full echo adds later. Each window opens a set of standard views the reader works through in turn, the chambers, the valves, and the great vessels each brought onto the screen in a fixed order so none is skipped.
Reading how the heart pumps
How well the heart squeezes is the reading the focused scan does best. A vet learns the look of a strong heart, the walls of the main pumping chamber driving inward hard and the chamber going small at the peak of each beat.
A number puts a figure on it. The fractional shortening measures how far the chamber narrows from its widest to its tightest, set out as a percentage. A healthy dog lands somewhere around a quarter to a little under a half, the exact range set by the breed. A figure well below that band points to a muscle losing its strength. The number leans on a clean measurement, the chamber caught at its widest and its tightest in the same beat, which is why a steady patient and a clear picture matter as much as the figure itself.
The eye and the number work together. A heart that looks sluggish and measures low is a heart whose pump is failing, the change that sends a coughing dog toward heart-failure treatment. The focused scan flags it. How far it has gone is for the full echo to settle.
A weak pump shows in more than the walls. The blood slows and swirls in a chamber that no longer empties, a smoke-like haze the eye picks up in a failing heart. The valves may flap loose in a chamber grown so wide the leaflets no longer meet. The scan reads these knock-on signs alongside the squeeze itself, each one another mark of a muscle giving way. The squeeze is read the same way on a cat or a horse, the numbers alone set by the size of the heart. A pony’s heart fills the screen where a kitten’s sits small and beats fast, the reader holding the healthy range for the species in mind.
The size of the four chambers
A heart under strain grows. The chamber that takes the strain stretches to hold more blood or to push against more resistance, and that stretch shows plainly on the scan. Reading chamber size is half of what a heart scan does.
The left atrium is the chamber a heart scan watches first. It sits just upstream of the main pumping chamber, and it swells early when pressure backs up behind a failing left heart. The scan measures it against the aorta beside it, the great vessel leaving the heart. A left atrium no larger than about one and a half times that aorta sits in the normal range. One grown well past it warns of a heart filling under pressure, the change that comes before fluid backs into the lungs. A swollen left atrium on a coughing dog is one of the findings a focused scan is run to catch, since it points the cough at the heart and away from the airways, and it marks the point where a watched murmur becomes a treated disease. The measurement takes only a frozen frame and a pair of calipers. It carries weight a stethoscope alone never reaches.
The main pumping chamber is measured too, its width read against the animal’s body weight so a Great Dane and a terrier are each judged on their own scale. A chamber stretched wide for the dog carries a muscle giving way under it.
Diseased heart muscle takes two broad shapes on the scan, a ventricle stretched wide with thinned walls, or a ventricle with walls thickened inward around a crowded chamber. Each is a disease in its own right, worked up and managed along its own lines, with its own page in this library.
The right side of the heart is read as well, for the strain that backs up from the lungs. A right side swollen and struggling points the search toward the lungs and the vessels that feed them. A bulging right heart with a swollen vein behind it is read for the lung disease, the clot, or the heart defect driving the back-pressure.
The cat’s heart
A cat’s heart asks more of the scanner. It is a small heart, beating fast, two or three times for every breath. A frightened cat drives it faster still. The reader works quickly between the ribs of a patient that will not hold a pose for long.
The disease the scan hunts hardest in cats thickens the heart wall inward, crowding the pumping chamber smaller. It can sit silent for years, the first sign a sudden crisis. A focused scan that reads a thickened wall in a cat sends it on for the full study that confirms the disease and its page in this library.
That crisis often arrives as a clot. A heart whose left atrium has swelled and slowed can throw a clot that lodges where the body’s main artery splits toward the hind legs, leaving a cat dragging them in sudden pain. A scan that catches the swollen atrium early is a scan that warns of the clot before it forms. A cat resents being held on its back, so its heart is read with the cat sitting up or on its side, the probe slipped between the ribs from below. The scan is kept short, a frightened cat’s racing heart reading poorly until it settles.
The young heart and its murmurs
A murmur in a young animal asks its own question. Many puppies and kittens carry a soft murmur that fades as they grow, the harmless flow of a fast young heart. A louder or lasting one can mark a heart built wrong from birth.
The scan tells the two apart. A soft murmur over a young heart that reads normal usually fades on its own. A narrowed valve, a hole between two chambers, a vessel that stayed open past birth: each shows on the scan as a fault the ear could only guess at.
Catching these early changes everything. A defect found in a pup gives an owner the choice to treat it, to plan around it, or to step back from a breeding line that carries it. A scan run on a litter’s murmur is a scan that shapes the years ahead.
A young animal’s heart can carry a murmur that time alone will clear, the kind a scan reads as harmless. The same scan separates that innocent flow from a defect that will only worsen, the reading that tells an owner whether to worry or to wait.
A focused scan triages, it does not crown
The focused scan sorts the urgent from the stable. Naming the disease is the cardiologist’s work.
The valves and their leaks
The four valves keep the blood moving one way. A valve that no longer seals lets a backward jet slip through with each beat, the leak behind many a murmur. The other valves can leak as well. Those leaks are the rarer ones. A leak on the right side, or a valve narrowed so the blood struggles through it, each leaves its own mark on the chamber it strains. The focused scan reads the strained chamber, leaving the full echo to name the valve.
The commonest is the mitral valve, the gate on the left side of the heart. In small breeds its leaflets thicken and curl with age until they no longer meet. The blood then leaks back into the left atrium. This worn-valve disease is the commonest heart trouble of the older small dog. The swollen left atrium it leaves behind is what the focused scan reads.
A loud murmur and a quiet one can both sit over a heart in trouble, so the scan reads the chambers behind the sound to weigh what it means. Seeing the leak itself takes colour flow, the Doppler that paints moving blood across the screen. A full echo lays this colour over each valve and times the jet with a second Doppler trace. Many handheld units carry only the grey moving picture, so the focused scan reads the leak through its mark on the chambers, leaving the colour study to the referral. A thickened, ragged valve flapping on the grey image still tells the reader a leak is there, even before the colour confirms it. The size of the chamber behind it shows how much blood the leak is losing.
Not every leak needs the colour study to be read. A valve worn thick, its edge ragged on the grey picture, a chamber swollen behind it, tells the reader enough to act, the colour left for the full echo to confirm the detail.
Fluid around the heart
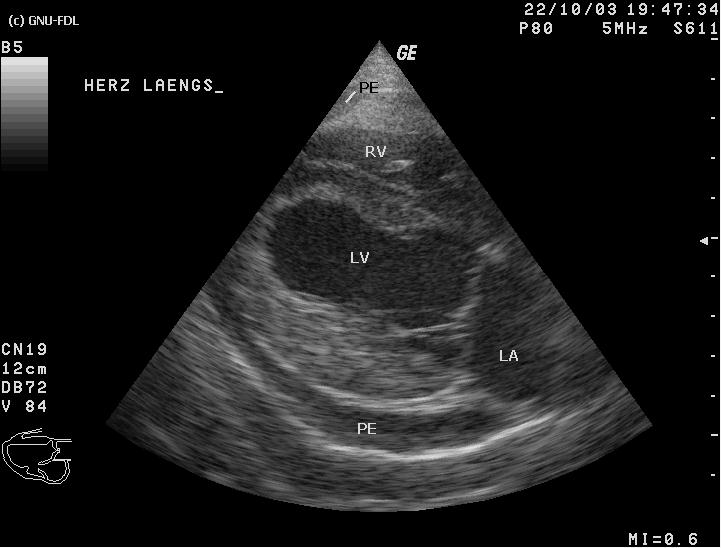
The heart sits in a thin sac. Fluid filling that sac shows on the scan as a black space wrapping the heart, clear against the grey muscle. A focused scan finds it fast, and a trained hand reads it with high accuracy, which is why this find is the one that brought cardiac ultrasound into the emergency room. The fluid comes of many causes, a bleeding tumour on the heart base, an inflamed sac, a clotting fault. The scan reads the heart wall and base for the mass that so often lies behind it.
Loose fluid in the sac is one thing to manage. The danger comes when there is enough of it to squeeze the heart from outside until the chambers cannot fill, a state called tamponade that drops the blood pressure and kills within hours. The scan reads the signs of it: the thin-walled right chambers buckling inward when they should be filling, and the big vein returning to the heart standing swollen, packed with blood it cannot push on.
A heart drowning in its own sac is drained at once. A needle passed into the sac under the watching probe pulls the fluid off and lets the heart fill again, a rescue the scan both calls for and guides. The relief can be immediate. The fluid drawn off is read in the syringe, its colour and content pointing to the cause, blood from a torn tumour, a clear seep, or the cloudy fluid of an infected sac.
The scan stays on the case afterward. A sac that fills again, or a mass on the heart wall feeding the bleed, is watched on the follow-up scans, the picture showing whether the trouble settles or builds.
What the focused scan hands on
A full echo reaches past the focused scan in two ways. An M-mode trace draws a single line through the heart and plots its motion against time, measuring wall thickness and chamber size to a fraction of a millimetre. Doppler reads the speed and direction of blood through every valve and across every chamber.
Together those tools build the complete picture, the one that names a specific muscle disease, grades a leak, and stages where a heart sits on the road to failure. That picture is the cardiologist’s work, often on a cart-based machine with a probe and software built for the heart.
The handheld earns its place ahead of that referral. It answers the bedside question, calls the emergency, and tells the vet which animal needs the specialist this week and which can be watched. A focused scan in the right hands turns a vague murmur into a clear next step. The two scans are partners, the focused look in the consult room and the full study in the cardiologist’s hands, each doing the part it does best.
Reading the rest of the picture
A heart never works alone, and the focused scan reaches a little past it. The big vein returning blood to the heart, read where it crosses the liver, tells how full the circulation is. A vein standing wide, holding its width through the breath, speaks of a heart struggling to keep up, or of a sac squeezing it from outside.
The lungs above the heart finish the picture. A heart failing on its left side floods the lungs. That flooding throws bright vertical lines across the lung surface, read on the same probe in the same minute. A vet who sees the swollen heart and the wet lung together holds the whole story of a breathless dog in one sitting.
One probe, the whole story
This wider look is what earns the handheld its place at the bedside. One probe reads the heart, the vessels, and the lungs. It turns a breathless animal into a working diagnosis without a step out of the room.
From the scan to the plan
A heart scan is read for what it changes. The picture is never the point on its own. A swollen left heart and a wet lung on a coughing dog send it home on a water tablet that pulls the fluid off the lungs. The scan is what tells a vet the cough belongs to the heart, the moment to start the drug.
The findings set the timing of the referral. A mild change under a soft murmur earns a watch and a rescan in a year. Each step up in what the scan shows, a chamber stretched hard, a fast-failing pump, a sac filling with fluid, shortens the road to the specialist and the full study. The amount of fluid in a sac matters less than the speed it gathered. A sac that fills fast gives the heart no time to adjust, choking it on even a small volume.
The scan also shapes the hard conversations. An owner shown the heart on the screen, the chamber stretched and the pump weak, takes in the road ahead in a way no spoken description reaches. The picture turns a diagnosis into something a family can see and plan around.
How the scan is run
The animal lies on its side, often on a table with a cutout that lets the probe reach up from below into the down side of the chest. The fur over the heart is clipped, and warm gel is worked into the skin. An animal left standing, or scanned through a thick unclipped coat, gives a softer, harder-to-read picture.
A clip from the ECG runs alongside the image on many machines, marking each beat against the heart’s electrical signal. That timing helps the reader catch a measurement at the right moment of the cycle. A calm patient holds still and breathes slow. A slow, steady heart reads far more cleanly than a racing, frightened one. Two people make the work easier, one holding the animal in a gentle, secure grip while the other drives the probe, the patient kept reassured through a few quiet minutes on its side.
What the focused scan can miss
The focused scan has real limits. An honest vet works inside them. A subtle muscle disease early on, a small leak, a chamber only slightly enlarged: these can slip past a quick grey-scale look that carries no Doppler and no fine measurement.
Even the emergency find has its traps. Tamponade can be hard to call on the picture alone. Readers disagree on the early signs of it. The scan is weighed with the animal in front of it, the pulse, the gums, the blood pressure, the picture only one piece of the call. A focused scan that cannot settle a question sends the animal on for the full study. It never calls a heart clear on a doubt. A scan run in a hurry, on a panting cat or through a thick coat, is the one that misses the early disease, which is why an honest reader notes a poor study and brings the animal back for a clearer one.
The picture the focused scan gives
What the focused scan gives is a decision the vet can act on within the hour. The vet who runs it walks away knowing whether the heart is the problem, whether it is an emergency, and whether the animal needs the specialist this week.
The reach of the scan grows with the hand that holds it. A practised vet pulls more from a pocket machine than a beginner pulls from a cart, the value in the reading more than the price of the probe.
None of it replaces the cardiologist’s full study. The handheld maps the ground and points the way toward it, leaving the specialist’s echo to fill in the detail the bedside scan leaves open.
A handheld heart scan turns a murmur, a faint, or a hard breath into a working answer. It reads the pump, the chambers, and the sac around the heart, calls the emergency, and hands the rest to the specialist with the ground already mapped.
Common questions about a heart scan
What can a handheld echo tell me about my pet’s heart?
It reads how well the heart is pumping, whether the chambers have stretched, and whether fluid has gathered around the heart. It is a focused scan that answers urgent questions and points to whether your pet needs a heart specialist. It does not give the full measurements and flow studies of a complete echocardiogram.
Can a focused scan diagnose the exact heart disease?
Not on its own. It sorts the urgent from the stable and turns up the big findings, a weak pump, a swollen chamber, fluid around the heart. Naming the specific disease and grading it takes a full echo with M-mode and Doppler, run by a cardiologist.
Why is fluid around the heart an emergency?
A sac filling with fluid can squeeze the heart until its chambers cannot fill, a state called tamponade that drops the blood pressure fast. The scan finds the fluid and the signs of pressure. A needle drained under the probe relieves it. Caught late, it kills within hours.
Which view does the heart scan use?
The main window sits low on the right chest wall, behind the elbow, where the heart leans against the body and the lung pulls clear. From there the probe takes a long view down the heart and a short cross-section across it. The left chest adds a window for the flow studies of a full echo.
Does my pet need to be sedated for a heart scan?
Many tolerate it awake, lying on their side with a clipped patch and warm gel. A calm patient with a slow steady heartbeat gives the cleanest picture. Gentle handling, and a light sedation now and then for a fractious one, settles a frightened animal enough to read.

About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.