Apical Four Chamber A4C View Handheld Echocardiography
The apical four-chamber view looks up through the tip of the heart and lays all four chambers open at once, the two ventricles below and the two atria above, the valves between them swinging in the middle of the screen. No other window sets the right ventricle directly beside the left for a fair comparison of their size; none reads the inflow of both valves in a single frame. It is the view a clinician turns to when the question is the right heart: is it swollen, is its wall moving, is it dragging the whole circulation down with it. The apex is harder to find than the parasternal spots, but the reading it gives back is among the richest a handheld probe can take.
Probe at the apex, marker to the patient’s left.
That placement, and its order in the wider sweep, sits in the overview of the standard windows. The rest is the four-chamber itself: how to read the right heart from it, where the apex hides its secrets, how a foreshortened image fakes a heart it is not looking at.
All four chambers at once
The view arranges the heart in a fixed pattern once the apex is found. The left ventricle and left atrium fall on one side of the screen, the right ventricle and right atrium on the other, the apex at the top where the probe sits and the two atria at the bottom. The mitral valve guards the left inflow, the tricuspid the right, the two of them side by side across the middle. The whole picture is drawn upside down from the way the heart sits, the apex at the top of the screen and the atria at the bottom, since the probe looks up from below the tip; a clinician who forgets that inversion reads the heart standing on its head and mistakes near for far.
One small offset names the sides for certain. The tricuspid valve sits a little closer to the apex than the mitral, its hinge planted slightly lower on the septum, so the valve that attaches nearer the tip marks the right side of the heart even when nothing else does. A clinician who reads that offset never confuses the chambers, a confusion that would turn a healthy heart into a frightening one.
The left side of the frame carries its own quick readings. The left ventricle forms the true apex and gives a second look at the pump the parasternal cuts began, its squeeze judged from a fresh angle; the left atrium below it, stretched wide, speaks of a pressure long backed up behind a stiff or leaking left heart. The four-chamber gathers both atria at the foot of the screen, where their size, so easy to skip past, records the slow history a single beat cannot show.
Four chambers, two valves, one frame.
On the four-chamber the right ventricle sits beside the left. Normally it is the smaller, reaching about two-thirds to the apex (left). Swollen to match the left and reaching the tip (right), it warns of strain. Original illustration.
The right ventricle, by size and by wall
The four-chamber view is the home of the right heart; it reads that chamber in ways the other windows cannot. The first reading is size, taken by eye against the left ventricle sitting right beside it. A healthy right ventricle is the smaller of the two, a slim triangle reaching perhaps two-thirds of the way to the apex, its neighbour the larger, rounder chamber that forms the true tip of the heart. Let the right ventricle swell until it matches the left in width at the base, or passes it, or shoulders its way down to form the apex itself: the eye reads a right heart under heavy strain, the size alone telling the tale in a breathless patient who may be throwing clots to the lungs. The view reads the wall as well as the width; here it offers a sign that sorts a sudden strain from an old one. In a fresh, massive clot to the lungs the right ventricle’s free wall, the long outer wall facing away from the septum, goes still and bulges as the tip of the right ventricle keeps contracting briskly, a pattern named after McConnell, the free wall down and the apex spared. That apical sparing points hard at an acute event over the slow grind of a long-standing pressure, which tends to drag the apex down with the rest. A third reading, taken with a single line of M-mode dropped on the outer hinge of the tricuspid valve, measures how far that hinge travels toward the apex with each beat; a generous travel means a right ventricle still pulling its length strongly, a feeble travel a right ventricle failing in its long direction. Size beside the left, a free wall that moves or does not, a tricuspid hinge that travels far or little: three readings of the right heart the four-chamber lays open that no lengthwise parasternal slice can frame, the shape of the septum being the short axis’s job and the bulk and motion of the chamber being this one’s.
A right ventricle as big as the left is a right ventricle in trouble.
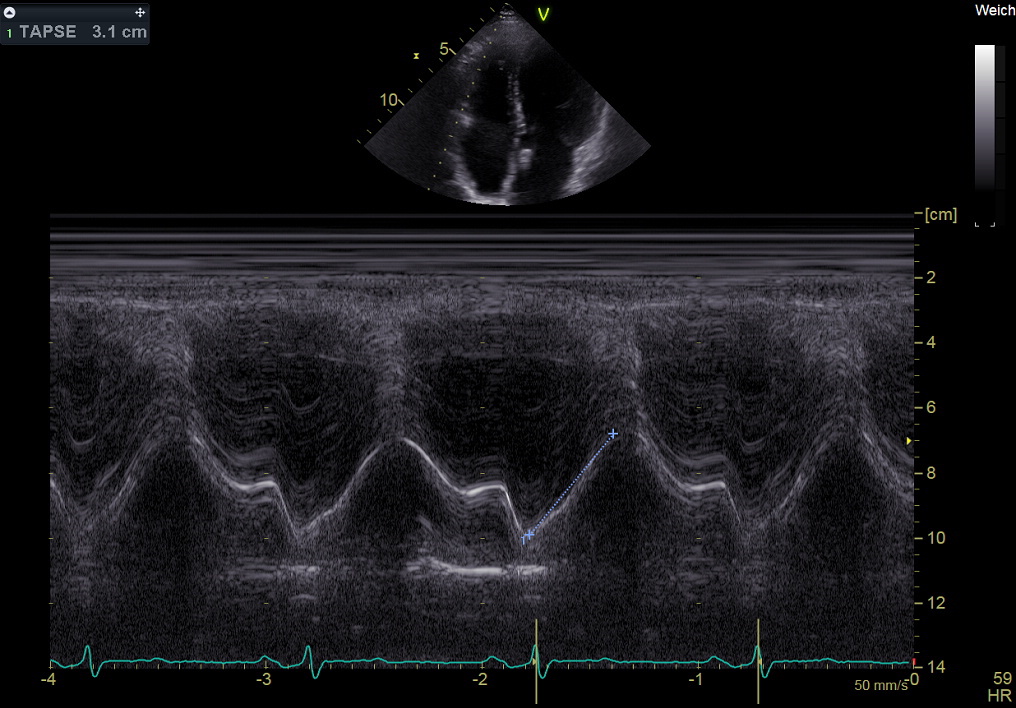
TAPSE: an M-mode line on the outer tricuspid hinge records how far it travels toward the apex each beat, a gauge of right-ventricular long-axis function. Wolff-BI, Wikimedia Commons, CC BY-SA 3.0.
The apex, where clots hide
The true tip of the left ventricle is a corner other views skim past; the four-chamber is built to reach it. A heart weakened over the front wall can balloon at the apex into a thinned, bulging pouch, and in the still eddy of blood that collects there a clot can form, a pale mass clinging to the tip that throws strokes if it breaks free. The apical view, aimed straight at that corner, is the one that catches it. The apex is also where a thickened heart can hide its worst, the muscle of a certain cardiomyopathy bulking at the tip into a shape the parasternal cuts foreshorten away; the four-chamber, aimed true, is the view that shows it.
The catch is that the apex is the easiest part to lose. Press the probe too high on the chest and the beam cuts across the heart short of its tip, a foreshortened image that chops the true apex off and shows a rounded false one. A clot sitting in the real apex hides above the edge of such an image, unseen, the foreshortened ventricle looking shorter and stronger than it is. The remedy is to chase the tip deliberately, sliding lower and more to the side until the ventricle lengthens and the apex sits at the top edge of the sector, then to study that corner on its own before reading anything else.
The corner the other views skip is the one a clot picks.
The inflow valves and the flow
The four-chamber frames both inflow valves cleanly, the mitral and the tricuspid opening toward the probe with each filling. Their leaflets are read for a full open and a tight close, a tethered or flailing leaflet showing against the smooth swing of a healthy one, the tricuspid checked for the displacement that marks a heart malformed from birth.
Colour laid over the valves adds the flow.
A tongue of colour chasing back into an atrium as the heart squeezes marks a valve that leaks, the mitral on the left or the tricuspid on the right; a strong tricuspid leak read here is itself a clue to the pressure straining the right heart. The same view aligns the beam straight down the inflow for the pulse-wave readings that gauge how stiffly the left ventricle fills, a depth of reading a focused exam touches lightly and a full study takes up in earnest. The speed of a tricuspid leak, caught here, even yields a number for the pressure in the lungs, the faster the backward jet the higher the pressure driving it, an estimate the full study leans on and the focused eye notes in passing. A leak that paints half the atrium with colour reads as large; a thin jet hugging the valve as trivial, the coarse grades a handheld scan is built to give.
Finding the true apex
The apex rewards patience and the right position more than force. Rolling the patient onto the left side drops the heart against the chest wall and brings its tip within reach, the single move that turns a hopeless apical window into a clear one. The probe then sits low and lateral, over the point where the beat is felt, aimed up through the tip toward the right shoulder instead of pressed flat against the ribs. A breath let halfway out and held drops the diaphragm and settles the heart into a steadier place, the moment the apex sits cleanest, and a slow scan along a rib space keeps the beam off the bone that would shadow the tip.
The shape of the ventricle tells whether the apex is true. A correct four-chamber shows the left ventricle as a long bullet, its walls tapering to a narrow tip; a foreshortened one shows a stubby, rounded chamber more like a ball. Fanning and sliding until the ventricle stretches to its longest bullet, with the tricuspid and mitral hinges both in view, is the sign the cut has reached the real apex rather than a slice across the body of the heart.
Hunt the long bullet, not the round ball.
Where it misleads
Foreshortening is the great deceiver of this view. A chopped apex shrinks the left ventricle, hides a clot or an aneurysm at the tip, flattering a failing pump into looking brisk, all from a probe held a rib too high. The size of the right ventricle, judged by eye, also swings with the angle of the cut, an off-axis slice fattening or slimming a chamber that a true four-chamber would size correctly. The single plane can miss a clot tucked behind a wall it never crosses, the reason the apex is swept slowly, the beam fanned through the whole tip before the corner is called clear.
The view is one plane of a moving organ; it reads best in company. A right ventricle that looks large is confirmed against the short axis and its septum; a doubtful apex is checked from a second angle; an eyeball pump read is weighed against the parasternal windows. The four-chamber is the richest of the focused views and the easiest to misread; the cure for both is the same: find the true apex, then read it alongside the rest.
Why it anchors the right-heart read
The four-chamber is where the right heart stops being an afterthought. A focused exam built only on the left-sided parasternal cuts can watch the pump and the valves and still miss a right ventricle swelling toward failure; the apical view sets that chamber beside the left, reads its wall and its long-axis pull, turning the right heart from a guess into a measurement any trained hand can take. In a breathless patient with clean lungs and a clear left ventricle, it is the four-chamber that often names the trouble. The lungs scanned clear, the left ventricle squeezing well, a wide and struggling right ventricle on the apical view points the search straight at the vessels, the clot in the lung that no left-sided cut would have caught.
The deeper value of the view is the story it tells in one frame. The size beside the left ventricle, the free wall that moves or stalls, the hinge that travels far or little, the apex held clear of foreshortening: read together they sketch the state of the right heart in seconds, a reading that once waited on a full study and now arrives with a probe laid on the tip of the heart and turned the right way. A right heart that once declared itself only on a scan down the corridor now shows its size and its struggle at the bedside, in the first minutes that decide a clot’s treatment. The tip of the heart is the hardest of the windows to find, and it repays the search with the fullest reading any of the five gives back, the right side and the left told in a single upward look.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.