Parasternal Long Axis PLAX View With Handheld Ultrasound Probe
The parasternal long axis is the view a clinician learns first and leans on hardest. It cuts the heart along its length and lays the left ventricle, the mitral valve, the aortic root and the left atrium across the screen in a single clean slice, the one picture that reads the pump and two valves at a glance. The placement is the easy half of the skill; the reading is where the view earns its keep, since a good long axis answers questions about strength, valves and the sac that no other window frames as plainly.
Probe at the left sternal edge, marker to the right shoulder.
That placement, and where the view sits in the wider sweep, is the smaller part of the skill. The reading that follows it is where the long axis repays the learning, the marks below being the ones the other windows never frame as plainly.
Three structures in one cut
The long axis is built around three landmarks stacked across the screen. At the centre sits the aortic root and the aortic valve, its thin leaflets opening to a box in time with each beat. To its left lies the left atrium, the chamber that fills behind the valve. Running through the middle is the mitral valve, its two leaflets swinging in the inflow between the atrium and the ventricle; below them lies the left ventricle, the thick-walled pump whose squeeze the view reads best of all. The three sit in a fixed relation on the screen, the aortic root pointing to the right, the apex trailing off to the left, a layout this constant that an image where they fall elsewhere is a sign the cut has gone oblique more than a sign of disease.
Each structure carries a question. The aortic valve is checked for a clean opening and a tight close; the mitral leaflets for free movement and a full seal; the left ventricle for the strength of its squeeze. The long axis sets all three in one frame, so a single steady image answers three questions at once, which is the deeper reason it leads the round.
The left atrium repays a second look the quicker scans skip. A chamber stretched wider than the aortic root beside it, the two read at a glance against each other in the one frame, speaks of a pressure long raised behind a stiff or leaking left heart, a chronic mark the long axis carries almost by accident. The aortic root in the same picture shows its calibre too, a root ballooned wide hinting at an aneurysm a focused eye can flag and a fuller study can measure.
On the long axis the descending aorta is the divider: pericardial fluid tracks in front of it, against the heart; pleural fluid tracks behind it. Original illustration.
The descending aorta, the line that sorts the fluid
The long axis hides a landmark that settles one of the commonest confusions in chest ultrasound; learning to find it is half the value of the view. Look behind the heart, just past the back wall of the left atrium near the groove where atrium meets ventricle; a small round dark circle sits there in cross-section: the descending thoracic aorta, the great vessel running down behind the heart. It looks like nothing of importance until fluid appears, and then it becomes the line that tells one kind of fluid from another. A pericardial effusion, fluid in the sac that wraps the heart, collects between the heart and that sac, so it tracks in front of the descending aorta, sliding in between the heart and the vessel; a pleural effusion, fluid in the space around the lung, collects outside the sac, so it tracks behind the descending aorta, pushed away from the heart by the vessel between them. The same dark stripe of fluid means two different things, two different treatments, depending on which side of that little circle it falls. A clinician who has fixed the descending aorta in the eye reads the answer in a second: fluid in front of it, think the sac and the squeeze of tamponade; fluid behind it, think the lung and a different path entirely. The view carries a second trap to name in the same breath. A thin dark band seen only in front of the heart, with nothing behind, is more often a pad of fat sitting on the heart than a true effusion, since real pericardial fluid in a patient lying flat pools first in the dependent space behind the left ventricle. A rim that shows behind the heart is the one to trust; a stripe that shows only in front is held in doubt until a posterior view confirms it. These two readings, the aorta that sorts pericardial from pleural and the dependent pooling that sorts fat from fluid, are the long axis at its sharpest. Neither is obvious to an eye that has not been told where to look.
Front of the aorta, the sac. Behind it, the lung.
Reading the pump without a number
The long axis reads left ventricular strength two ways, neither needing a measurement. The first is the plain eyeball: watch the walls thicken and the cavity shrink with each beat; judge the squeeze strong, fair or weak the way one judges a fist clenching. A vigorous ventricle nearly obliterates its own cavity at the peak of the beat; a failing one barely changes size, the walls slack and the chamber wide through the whole cycle. The long axis catches the front wall and the back wall of the ventricle in the one slice; a segment that thickens as its neighbour lies still betrays an old injury to a single wall, a regional weakness the global eyeball would otherwise average away.
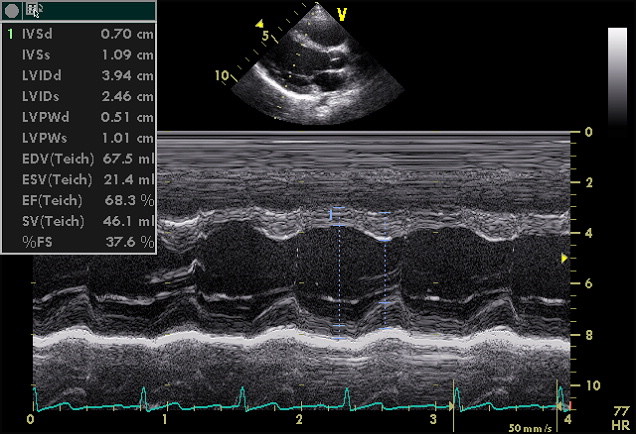
An M-mode tracing through the long axis, the mode that times wall motion and the mitral leaflet against the septum. Wikimedia Commons, public domain.
The second is a small, sharp trick the view offers for free. The front leaflet of the mitral valve, swinging open in early filling, normally flicks up almost to touch the wall of the septum just in front of it. A vigorous heart brings them nearly together; a weak, dilated heart leaves a visible gap between the leaflet’s tip and the septum. That gap, the distance the leaflet falls short, tracks the strength of the pump closely enough that a wide one flags a poor ventricle at a glance, a number-free reading any trained eye can take from the long axis in seconds.
The leaflet trick has its bounds. A stiff or leaking mitral valve moves on its own rules, the gap no longer tracking the pump; a heart thickened by long pressure can squeeze hard in the long axis and still fail in ways this slice never shows. The reading is a quick proxy, trusted alongside the eyeball and checked against the other windows; it is no measurement to hang a whole verdict on.
The valves seen plainly
The long axis frames two valves better than any other quick view. The aortic valve sits side-on, its leaflets opening to a clean box and closing to a single line; leaflets that fail to open fully, or that flutter and leak, show their trouble here first. The mitral valve swings in the same frame, its leaflets read for a full open and a tight close, a flail or a thickened, tethered leaflet standing out against the smooth motion of a healthy one.
The view shows gross valve trouble, not fine grades.
A handheld scan does not pretend to grade a leak or measure a narrowing the way a full study does. It catches the large, plain faults: a valve that barely opens, a leaflet that swings loose, a jet of colour where blood escapes the wrong way. Those gross findings, seen on the long axis, are often enough to send a patient toward the fuller study that measures what the focused view only flags.
The colour mode many handheld probes carry adds a layer the grey alone misses. On the long axis a tongue of colour licking back into the left atrium as the heart squeezes marks a leaking mitral valve; a spray below the aortic valve as the heart fills marks a leaking aortic one. The colour shows that a leak is there and roughly how it runs, the grading of how badly left to the cart and the cardiologist.
Getting a true long axis
A good long axis is harder to obtain than to read; the early errors are errors of angle. The cut must run truly along the length of the heart, through the centre of the aortic and mitral valves; a probe rolled even slightly off that line gives an oblique slice that shrinks the ventricle, blurs the valves and fakes findings that are not there. The fix is patient fanning: small tilts and slides until the aortic valve and the mitral valve sit at their widest and the ventricle stretches to its longest, the sign that the beam has found the true long axis.
Depth and gain matter as much as angle. The view is set deep enough to show the descending aorta behind the heart, since that landmark is lost if the image stops at the back wall of the atrium. The gain is set so the blood in the chambers reads black and the walls read bright, the contrast that lets a thin rim of fluid or a slack wall show itself rather than wash into grey.
The patient helps or hinders the view. Rolling them onto the left side brings the heart against the chest wall and out from behind the breastbone, opening a window a flat-on-the-back position can bury, a small move that rescues many a poor parasternal image. A held breath in gentle exhalation steadies the heart against the drift of the lungs, the moment to freeze a clip or take the reading.
Fan until the valves are widest; that is the true axis.
Where it misleads
The long axis has its blind spots like any single view. It sees only a thin slice, so a wall problem off the plane of the cut can sit unseen while the slice itself looks normal. It judges the pump from one angle; an eyeball estimate taken from a foreshortened or oblique image can read a normal heart as weak or a weak one as fair. The view is a strong first look, never the whole reading.
A clot at the far tip of the heart, a fault in the lowest part of the septum, a valve lesion that faces away from the slice: each can hide from a perfect long axis, caught only when the probe moves on to the apical and short-axis windows that look from other sides.
The fat-pad trap and the oblique cut catch beginners more than the rest. A stripe of fat read as effusion sends a clinician hunting a problem that is not there; an off-axis slice read as a small, vigorous ventricle hides a heart that a true cut would show failing. Both are undone by the same discipline: fan for the true axis, look behind the heart as well as in front, and confirm a doubtful finding from a second window before trusting it.
Why it leads the sweep
The long axis earns its place at the front of the round by how much it settles in one image. A clinician who has just laid the probe on a breathless chest reads, in that first frame, whether the pump is strong, whether the big valves move, whether fluid sits in the sac, and on which side of the descending aorta any fluid falls. Few single views carry that much, which is why the long axis is the one a learner drills first and the one a crashing patient gets first.
The deeper lesson is that the view rewards the eye that knows where to look. The placement is quickly learned; the descending aorta, the leaflet gap, the dependent pooling are the readings that turn a clear picture into an answer. A long axis found and not read for those marks is a picture wasted; a long axis read for all of them is among the best few seconds a handheld probe can spend on a chest. The view repays a lifetime of small refinements, each scan teaching the eye a little more of what the single slice holds.
About the Author
Julien Mercier
Senior R&D Engineer · Medical Ultrasound Transducer Development
Senior R&D Engineer with an M.S. in Applied Physics and over 15 years of experience in medical ultrasound transducer development, specializing in the design verification and performance testing of high-frequency imaging transducers. Currently leading the development and verification of the company’s next-generation high-frequency linear-array transducer, responsible for imaging performance evaluation and reliability analysis in preclinical testing. Brings extensive hands-on experience in piezoelectric element tuning, beamforming parameter optimization, and system-level performance testing.