Liver Mass Tumor Ultrasound Differentiation Handheld Imaging
A liver mass on handheld ultrasound is read in two parts: the part B-mode can call with confidence, and the part it cannot. The split has a sharp boundary. A hemangioma with a textbook pattern declares itself in ten seconds; a heterogeneous nodule in a cirrhotic liver tells a much more guarded story. Knowing where the boundary sits is the difference between a useful report and a misleading one. The handheld probe finds the mass; it does not always finish the work. The job at the bedside is to call what can be called, flag what cannot, and write the next imaging step into the note before the patient leaves the room.
The masses that name themselves
The hepatic hemangioma is the easy one. A small, well-defined, uniformly hyperechoic lesion sitting inside otherwise normal liver parenchyma reads as a hemangioma at high probability with B-mode alone. The classic small cavernous hemangioma is rounded, sometimes lobulated at the edges, and brighter than the surrounding tissue at a similar depth. Posterior acoustic enhancement is variable. The lesion does not invade vessels, does not distort the capsule, and does not pulse. The handheld call is acceptable when the picture is textbook.
The simple hepatic cyst is the other lesion that names itself. An anechoic round structure with a thin smooth wall, posterior enhancement, and no internal echoes is a simple cyst at near-certainty on B-mode. Walls thicker than a millimeter, internal septations, debris, or wall nodules push the call from simple cyst toward complex cyst or hydatid disease and shift the answer outside what handheld B-mode alone can settle. The threshold is set by what is missing.
The masses that hide their identity
Hepatocellular carcinoma in a cirrhotic background is the lesion B-mode characterizes worst. The tumor can read as hypoechoic, hyperechoic, or mixed; it can be uniform or heterogeneous; it can have a thin capsule or no capsule; it can sit anywhere from millimeter nodule to lobar mass. None of these B-mode features is specific. A nodule above 1 cm in a known cirrhotic liver is a triage finding, not a diagnosis. The recommendation pathway is the same: contrast-enhanced ultrasound, multiphase CT, or contrast MRI before any HCC label is applied.
Metastatic lesions to the liver carry their own pattern vocabulary, none of which is reliably diagnostic alone. The classic finding is a hypoechoic mass with a hypoechoic peripheral halo, sometimes with a hyperechoic center, giving a target appearance. Multiple lesions favor metastasis over primary tumor; a single lesion does not exclude it. Calcifications point toward mucinous gastrointestinal primaries; cystic transformation points toward sarcoma or treated melanoma. The handheld call moves to a description of pattern, distribution, and number, not to a histologic name.
Focal nodular hyperplasia and hepatocellular adenoma cluster together in young women on contraceptives and overlap on B-mode. FNH is often nearly isoechoic with a faint central scar that handheld imaging rarely resolves; adenoma is more variable and can hemorrhage. Neither lesion answers to B-mode pattern alone. The call from the handheld is the size, location, and the fact of the mass; the differentiation belongs to CEUS or contrast MRI with hepatobiliary phase.
Several non-tumor entities mimic mass lesions and trap the inattentive scan. Hepatic abscess shows as a heterogeneous fluid-containing lesion with thick irregular walls and may contain debris or gas; the clinical setting of fever and elevated white count usually leads the read. Hematoma after trauma evolves through hyperechoic to hypoechoic to anechoic over days and weeks. Focal fatty sparing inside a fatty liver looks like a hypoechoic mass adjacent to the gallbladder or porta hepatis but follows vessels rather than displacing them. None of these is a tumor; all of them get read as one at the wrong moment.
Why the handheld stops short
The handheld convex probe at 3.5 to 5 MHz is built to find structures and outline them; it is not built to read what those structures are made of. Tissue characterization on B-mode alone depends on a small number of acoustic features: echogenicity, internal architecture, posterior enhancement or shadowing, presence of a capsule or halo, and the way the lesion deforms or fails to deform under transducer pressure. These features overlap heavily across diagnoses, and the overlap is the wall. A 2 cm hyperechoic nodule in a non-cirrhotic liver is statistically dominated by hemangioma, but small HCCs, focal fatty change, regenerative nodules, and hepatic adenomas can all read hyperechoic at this size and depth. Studies comparing B-mode characterization of indeterminate liver lesions against pathology consistently land in the 60 to 75 percent range for definitive characterization without contrast, and the missing 25 to 40 percent is not a matter of operator skill or sharper images. The information is not present in the signal. Cart-based scanners with contrast-enhanced ultrasound capability cross this wall by injecting a microbubble agent and watching the lesion fill and wash out over the arterial, portal, and late phases. The handheld has no contrast pump and no real-time phase imaging; the agent and the multi-phase workflow are not part of the device. Tissue harmonic imaging, which on cart-based machines lifts low-contrast lesions out of background speckle by reading only the harmonic returns and rejecting fundamental noise, sits at a much lower fidelity on many handhelds because the processing budget for harmonic extraction is constrained. Spatial compounding, which on cart-based machines averages multiple steering angles to suppress speckle and sharpen lesion edges, is absent or simplified on handheld platforms. None of these are settings to turn on; they are architectural choices made when the handheld traded acoustic infrastructure for pocket size. The consequence at the bedside is that some lesions look exactly the same on the handheld as they do on a cart machine, while other lesions look like undifferentiated blobs on the handheld and like clearly characterized hemangiomas, FNHs, or HCCs on the cart machine after contrast. A careful operator learns where the boundary falls for the device in hand and stops pushing past it. The wall is fundamental, not a knob to turn, and the report that respects the wall is the one the radiologist downstream can use. Pushing past it produces reports that read confident on the screen and contradictory in the chart when the contrast study returns the next day.
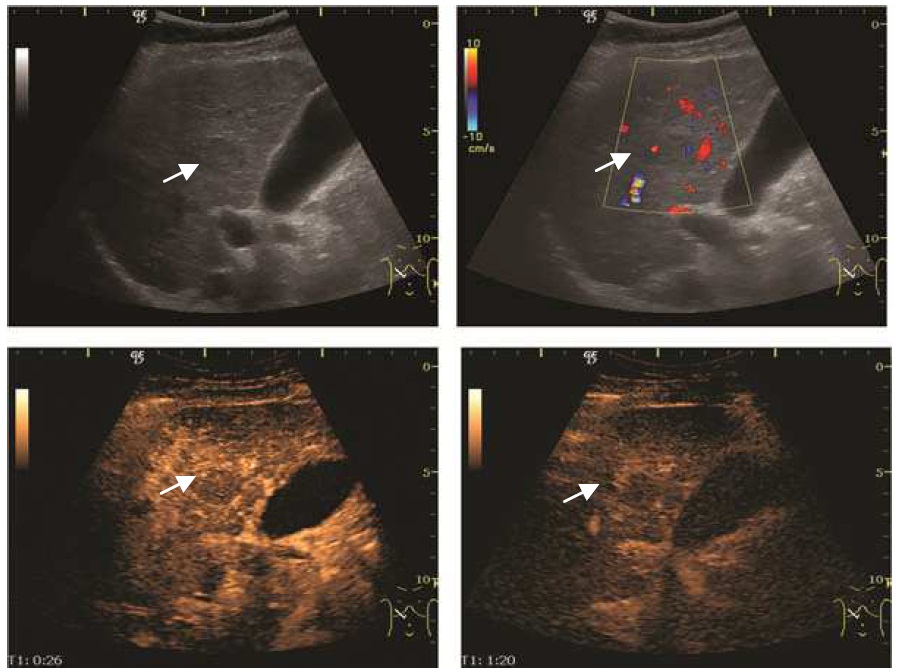
Color Doppler on B-mode helps but does not bridge the gap. Hemangiomas often show minimal internal flow despite their hyperechoic appearance; HCCs frequently demonstrate a feeding artery with a characteristic basket-pattern of intratumoral vessels; FNHs classically show a central feeding vessel with peripheral spoke-wheel branching. These patterns are real, suggestive, and helpful when present. They are also frequently absent on handheld Doppler because the wall filter, frame rate, and sensitivity to slow flow in small intratumoral vessels are weaker on handheld electronics than on cart-based ones. Useful when seen; the absence reads as nothing.
Tissue harmonic imaging at the handheld level is sometimes labeled in the menu and sometimes absent. The visible improvement, when the feature is present, is real but modest compared to cart-based machines that built dedicated harmonic processing into the beam-former. The label on the screen is not the same as the silicon behind it.
Spatial compounding on a cart-based array steers the transmit beam through multiple angles and averages the returning frames to reduce speckle and sharpen edges. The result is a visibly cleaner liver, with lesion borders that read as continuous rather than dotted. Handhelds either skip this feature outright or implement a lighter version that does not produce the same lift. The lesion edge that looks crisp on the cart looks granular on the handheld, and the call that hinges on edge clarity should be flagged.
Depth is the other handheld limitation that bites in liver work. A lesion in segment 7 or 8 close to the diaphragm in a tall patient can sit at 14 to 16 cm of tissue column from the right intercostal window, near the edge of the handheld’s useful penetration. The lesion appears, but the contour blurs and small features inside it dissolve into the far-field noise. Right lateral decubitus and the standard rib-window maneuvers help, but the deep posterior segments often remain the segments where the handheld answers least confidently.
Look
Look at what the screen does not say.
What you can call and what you cannot

There is a smaller list of lesions B-mode characterizes well enough to call. A textbook small cavernous hemangioma in a non-cirrhotic liver, a simple anechoic cyst with all the supporting features, a target-pattern metastasis with appropriate clinical context, and a known infantile hemangioma in serial follow-up all sit inside what the handheld can call without escalation. The list is short, and being inside it requires the textbook picture, not the close-enough picture. Drift from the textbook is the first signal to escalate.
The longer list belongs to indeterminate. A hyperechoic nodule above 3 cm, any lesion in a cirrhotic background, any solid lesion in a patient with a known extrahepatic primary, any complex cystic lesion, any rapidly changing lesion on serial scans, and any lesion with vascular invasion read as findings that require CEUS or contrast MRI before a tissue label is applied. The handheld call inside this set is descriptive: size, location by segment, internal pattern, vascularity if visualized, and a clean note that says contrast study or biopsy is the next step. Naming the lesion at this stage is the trap.
Reporting language carries the call. A lesion compatible with hemangioma reads differently from a hyperechoic lesion in segment 6, awaiting contrast characterization. The first carries an opinion; the second carries an observation and a next step. The report that lists features, pattern, and an honest probability range is the one a radiologist downstream can build on. The report that overcalls or undercalls forces the next reader to start from zero.
The next test, not the answer
The handheld scan finds the mass. That is the job in front of it. A liver mass on the screen at the bedside answers the binary question of whether something solid or cystic sits in the liver tonight; it does not answer the follow-up question of what that something is. Treating the handheld answer as the final answer collapses the workup into a single instrument and pretends a wall is not there. Treating it as the first answer in a sequence places it correctly: the handheld finds, the cart with contrast characterizes, and tissue sampling resolves what imaging cannot. Each instrument has its part. The handheld owns the first part.
The note that closes the bedside scan should carry four pieces. The fact of the lesion. Its location by segment and depth from the body wall. Its B-mode pattern, including size in two planes and any Doppler findings. And a one-line statement of what the handheld cannot settle, with the suggested next step. The downstream imager opens the report and knows what the patient has been through and what the patient still needs. The report that records absence as well as presence is the report that earns trust over time.