Splenomegaly Ultrasound Assessment Handheld Convex Probe
Adult splenomegaly is the abdominal finding handhelds miss more often than they should, and the reason is geometry rather than pathology. The spleen ducks behind the lower ribs, behind the stomach’s air, and behind enough body wall that a 5 MHz convex element runs out of useful penetration before it reaches the back of the organ. A scanner who walks into the room expecting to lay the probe on the flank and read the spleen in one window will overlook half the enlarged spleens in front of him. The fix is not a different machine; it is a different position, a deeper breath, and a different stretch of ribs to angle through.
The spleen behind the ninth rib
The spleen is wedged into the posterior left upper quadrant under the dome of the diaphragm, tucked between the 9th and 11th ribs. Its hilum opens forward toward the stomach; its convex surface presses against the diaphragm. From the body wall the organ is held away from the probe by a layer of intercostal muscle, two cortical bone shadows, and a variable wedge of stomach gas that shifts with every meal. None of these layers help the imaging. The acoustic window is not a window so much as a series of narrow slots between bone.
For the surface probe this matters less when the spleen is small. A 9 cm organ hides under the costal margin and the intercostal scan picks it up easily. Enlargement changes the geometry. As the inferior tip drops past the costal margin into the flank, the body of the spleen pushes posteriorly into a deeper plane and the upper pole crowds further under the rib cage. The bigger the spleen, the harder the spleen, even though intuition suggests the opposite.
How big is big enough
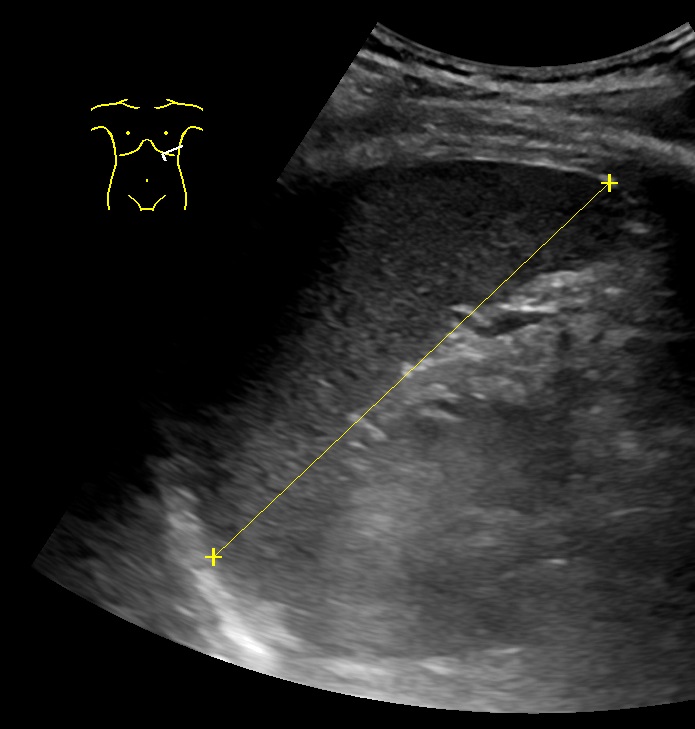
Adult cutoffs cluster around 11 to 13 cm in long-axis craniocaudal length. Different lab cultures pick different numbers within that band. The 12 cm figure gets quoted in textbooks; some societies prefer 11; some accept up to 13 in tall men. The number on the screen is less interesting than the band the patient falls into. A 14 cm spleen is enlarged in any framework; a 12 cm spleen in a 195 cm man is not necessarily abnormal.
Length is the easy number. Two other measurements travel with it: maximum width at the hilum and anteroposterior thickness. A normal spleen runs around 7 cm wide and around 4 cm thick at the hilum. A spleen that is long but thin is not as concerning as a spleen that has expanded in all three dimensions. The latter pattern, sometimes called isotropic enlargement, tracks reliably with disease.
Pediatric cutoffs scale with body length, not age. A useful rule of thumb is roughly 1 cm of splenic length per year of age up to about age 12, with hedged ranges around the mean for each year band. For neonates the upper bound sits around 6 cm. These pediatric numbers are softer than the adult numbers and any chart should be read alongside the child’s percentile for height, since a spleen at the upper edge in a tall child means something different from the same number in a small child. A spleen above the upper bound is suggestive, not diagnostic.
The single-measurement trap is the easiest one to fall into. The spleen needs to be measured in two orthogonal planes before anyone calls the size. A coronal length read from a single intercostal slice can be off by 1 to 2 cm depending on probe angulation. Check the number against a second window.
Why the handheld runs out of depth

A handheld convex probe at 3.5 to 5 MHz is asked to do something its physics resist. Acoustic penetration in soft tissue drops roughly with the inverse square of frequency, and the absorbed energy converts into heat rather than echo at the rates the imaging electronics can reconstruct. At 5 MHz the useful depth in average adult abdominal tissue lands somewhere around 14 to 16 cm before the signal returns become too weak for the time-gain compensation to recover them as usable image data. Cart-based abdominal arrays often run lower, around 2.5 to 3.5 MHz, with higher transmit power and a richer beam-former that handles the far-field returns more aggressively. The handheld probe trades that depth budget for portability. For a normal-sized spleen the trade is invisible; the organ sits comfortably inside the depth window. For an enlarged spleen of 16 cm or more, the back of the organ pushes against the edge of the handheld’s useful range, the posterior contour blurs, and the inferior tip in the flank window starts to drop below the horizon of the image at standard depth settings. The temptation in this moment is to push the depth slider further, sometimes past 18 cm, in the hope that the spleen will reappear. It does, after a fashion, but at the cost of axial resolution and frame rate. The picture turns gray and slow and the diagnostic value collapses with it. A better lever is the position of the patient, not the slider on the screen, because right lateral decubitus shifts the spleen anteriorly and inferiorly, the bowel falls away from the LUQ, and the same probe now reaches the same anatomy through a shorter tissue column. The depth budget that was insufficient in supine becomes sufficient in lateral, without changing the machine. The geometry of the change is straightforward. In supine, the spleen sits at a depth of around 14 to 18 cm from the body wall at the mid-axillary line; in right lateral decubitus, that distance drops to around 10 to 14 cm because the organ rolls forward with gravity and the rib cage rotates with it. A drop of 4 cm in tissue column is a substantial increase in returning echo intensity, often equivalent to a 6 to 10 dB improvement in signal-to-noise at the far field of the image. This is the single largest operator-side improvement in handheld splenic imaging, and it is invisible from any specification sheet.
Beyond the position, the intercostal angle is the second variable. The probe enters the chest wall through the 9th or 10th intercostal space along the mid-axillary line, with the index marker pointing toward the patient’s head. A 15 to 30 degree posterior tilt off vertical brings the long axis of the spleen into the imaging plane in a way that a strictly transverse cut cannot reach. Rib shadows fence the image on either side; the trick is to tilt the probe to thread a window between them rather than push harder against the bone. Pressure does not open the rib shadow. Angulation does.
Breath-hold opens the third lever. A deep inspiration drops the diaphragm a few centimeters, the spleen comes down with it, and the part of the organ previously hidden behind the costophrenic recess emerges into the intercostal window. The patient who can hold a deep breath for 3 to 5 seconds gives the cleanest images.
Arm position is the fourth lever and the one operators tend to forget. The left arm overhead, behind the head, opens the intercostal spaces by some 5 to 10 millimeters and changes the geometry of the rib cage enough that probes previously blocked by ribs now slide between them. The combination of right lateral decubitus, arm overhead, and a deep inspiration is the standard splenomegaly maneuver in formal ultrasound suites for a reason.
The TGC sliders deserve a careful pass once the position is set. The far-field returns from a deep spleen are weak and need the lower bank of TGC controls pushed up to recover them as visible echoes. Auto-optimization on many handhelds handles the near and middle field well but tends to underweight the deepest returns. A manual TGC pass aimed at the bottom third of the screen recovers the posterior splenic contour that auto-mode flattens into shadow.
Look
The contour comes into view, smoother than the kidney beside it, darker than the liver.
What the size brings with it
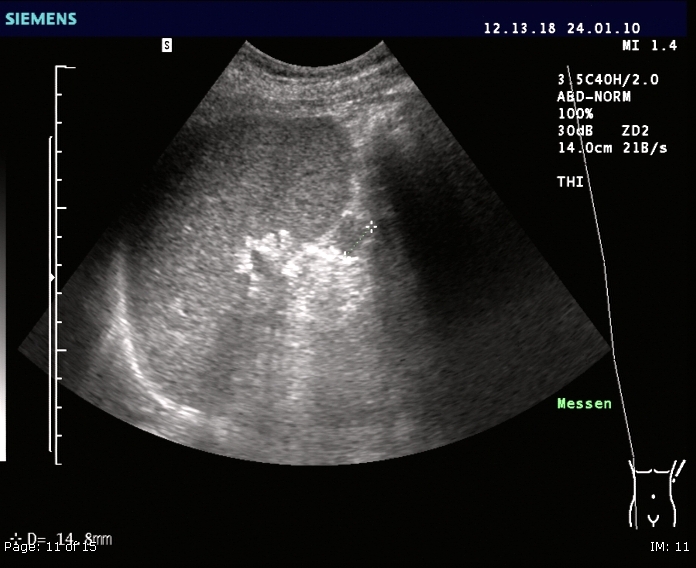
Splenomegaly without dilated vessels is one disease pattern. Splenomegaly with a dilated splenic vein and a dilated portal vein is a different disease pattern. The splenic vein at the hilum normally runs around 8 millimeters in diameter and varies a little with respiration. A splenic vein above 10 mm that does not change with breathing is a flag for portal hypertension, even before the liver itself is fully assessed. The vein is easier to see in lateral decubitus than supine; Color Doppler confirms the flow direction and whether reversal has occurred.
Splenic infarcts show as wedge-shaped hypoechoic regions extending from the capsule toward the hilum, with the broad base at the periphery. Fresh infarcts may be subtly hypoechoic and easy to miss; older infarcts retract into hyperechoic scar tissue and can mimic small calcifications. An infarct in the setting of new-onset splenomegaly should raise the question of a thromboembolic source, including atrial fibrillation, endocarditis, or a hypercoagulable state. When the size is borderline and an unexplained infarct is found, the borderline call usually swings toward calling the size pathologic.
Accessory spleens are common, found near the hilum or along the pancreatic tail, usually under 2 cm and rounded with the same echotexture as the parent organ. They become clinically relevant when a splenectomy patient develops persistent thrombocytopenia and an accessory spleen has been left behind. On a handheld these small nodules are easy to overlook, especially when the main spleen is enlarged and dominates the screen. The reading habit that catches them is a quick hilar sweep after the size measurement.
When the number turns into a diagnosis
Size on its own does not give a diagnosis. It points the workup. A spleen between 13 and 16 cm in an adult with chronic liver disease points one way; the same size in a febrile patient with weight loss and an HIV history points another. A spleen above 20 cm is rare and short-lists into the lymphomas, the chronic myeloid disorders, infiltrative infections like visceral leishmaniasis, and a small set of storage diseases. The handheld scan that finds the enlargement does not need to make the diagnosis; it needs to communicate the size and the accompanying findings clearly enough that the next step is unambiguous.
The clinical context is part of the read. Without context, a 14 cm spleen is a number on a screen. With context, it is a finding that reorganizes the differential, narrows the labs that need to be sent, and pushes the imaging workup toward the next step, whether that is a contrast study, a CT, or a repeat ultrasound in 4 to 6 weeks. The handheld is the entry point of the workup, not the destination, and reading it as the entry point means writing the size, the vessel measurements, and the pattern of enlargement into the note so that the next reader does not have to repeat the LUQ scan to know what was already seen.