Advanced Cardiac Evaluation Handheld Echocardiography
The focused exam answers the heart’s big questions by eye: is it pumping, is it strained, is the sac full, is the tank dry. Advanced evaluation goes a step further and puts numbers where the eyeball left impressions, measuring how much blood the heart moves with each beat, how high the pressure stands behind it, whether a litre of fluid would help or drown the patient. Those numbers come from Doppler, the trick of reading the speed of moving blood from the shift in the echoes it returns, a layer of the exam the quick eyeball look skips. A handheld probe can reach part of the way into that layer, and knowing how far it reaches, and where it must hand the work to a fuller machine, is the craft of advanced scanning at the bedside.
Numbers begin where the eyeball ends.
Finding the windows and reading the heart by eye sit in the pages on the individual views. The work here is the measured layer above that: the flow, the pressures, the dynamic tests, the limits a pocket machine sets on all of them.
From eyeball to number
A measurement earns its place only when it changes what happens next. The eyeball read of a pumping heart is enough for the bulk of decisions; reaching for a number makes sense when the question is finer, a borderline volume call, a filling pressure that decides a diuretic, an output trend across a resuscitation. The skill is knowing which questions deserve the extra minutes a measurement costs. Not every pocket scanner can take these numbers at all: the simplest show only the grey picture and a wash of colour, the better ones add the spectral trace the stroke distance needs, a few the tissue reading the filling pressure needs. Knowing which modes a given machine carries is the first step, since a measurement the device cannot make is one to leave to a machine that can.
The danger of a number is that it looks certain. A figure carried off the screen wears an authority an impression never claims; a poorly taken measurement, off-angle or read from one bad beat, lends false confidence to a wrong answer. A number is trusted only as much as the care that took it; on a handheld, with its simpler tools, that care has to be greater still.
Measure when the number will change the plan.
The stroke distance and the output
The number a Doppler scan adds with the longest reach is a measure of how much blood the heart ejects with each beat, and the way it is taken rewards a careful hand. Place the pulse-wave Doppler gate in the outflow tract of the left ventricle, just below the aortic valve; the machine plots the speed of the blood leaving the heart through each beat, drawing an envelope that rises to a peak and falls. The area under that envelope, traced by hand or by the machine, is the velocity-time integral, a length clinicians call the stroke distance: the distance a column of blood travels with one beat, normally somewhere near twenty centimetres. Multiply that distance by the area of the outflow tract and the result is the stroke volume, the millilitres pumped per beat; multiply again by the rate and the output of the whole heart falls out, a figure the eyeball can only guess at. The real power, though, is not the single number but the way it moves. Raise the patient’s legs to tip a bolus of their own blood back toward the heart, or run in a small fluid challenge, and watch the stroke distance: if it climbs by more than a tenth, the heart was sitting on the steep part of its curve and will pump more when filled, so fluid will help; if it barely stirs, the heart is already full and more fluid will only flood the lungs. That dynamic test, the stroke distance read before and after a reversible fluid shift, answers the question of whether to give fluid more truthfully than any still picture of a vein, since it asks the heart directly what another litre would do. A clinician who can take a clean stroke distance and read how it shifts with a leg raise holds the strongest quantitative tool the focused exam offers, the measure that turns the guess of how much fluid into a tested answer. The number is only as good as the trace behind it: the gate sits in the same spot each time, the beam lined up with the outflow, the envelope clean and free of the spray of a leaking valve that would corrupt it; a sloppy trace gives a confident, wrong figure. The trend matters more than the single value, the same patient measured the same way before and after a change telling more than one reading held against a textbook number.
Watch the stroke distance rise, or not, when the legs go up.
Reading the filling pressure
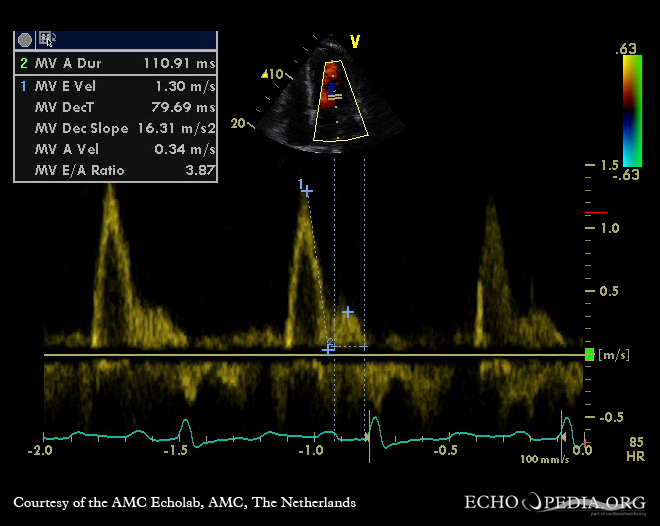
A second number reads the pressure at which the left ventricle fills, the gauge of a stiff heart. The Doppler gate set at the tips of the mitral leaflets catches the rush of blood into the ventricle in early filling, a velocity called E. The same gate, switched to read the slow tissue of the valve ring as it recoils, catches a velocity called e prime, the speed the muscle relaxes at. The ratio of the two, E over e prime, rises as the ventricle stiffens and the pressure needed to fill it climbs.
A high ratio points at a heart filling under a high pressure it cannot shed.
That reading matters: it names a kind of heart failure the squeeze alone misses. A ventricle can pump strongly yet fill so stiffly that the pressure backs up into the lungs, a failure of relaxation rather than of contraction, the breathless patient whose pump looks normal on the eyeball read. The filling-pressure number catches that stiff heart where the squeeze does not, adding a dimension the basic exam cannot reach, the difference between a heart that cannot push and a heart that cannot loosen. The ratio is read with the caution every Doppler number earns: it shifts with age, with the rhythm, with a leaking or stiffened mitral valve that throws the inflow off; it is taken as one pointer toward a high filling pressure, never a verdict on its own. In a breathless patient with a strong-looking pump, though, a high ratio is the finding that names the stiff heart the eyeball would have called normal.
What the handheld cannot do well
The pocket machine reaches into this layer only so far. Many handheld probes carry colour flow but a thin or absent spectral Doppler, with tissue Doppler thinner still, leaving the stroke distance and the filling-pressure ratio that need those modes beyond a given pocket device entirely. The advanced reading often waits, then, for a machine with the modes the handheld lacks. A clinician who reaches for the stroke distance on a device built only for grey-scale and colour finds the mode missing and the measurement impossible, the limit set by the hardware in the hand and not the operator’s skill.
Some readings belong wholly to the cart and the lab. The fine tracking of the muscle’s deformation through the beat, the strain that catches a weakening before the squeeze fails, needs software and a cart-based machine. The bubble study that hunts a hole between the chambers, the precise grading of a leak or a narrowing, the three-dimensional reconstruction of a valve: each is the work of the full laboratory, the sonographer and the cardiologist, beyond anything a probe in a pocket attempts. The handheld extends the bedside reach toward these readings; it does not replace the study that takes them properly.
The pocket reaches; the cart arrives.
The order of a measured study
The measured exam runs in a sensible order, the eyeball first and the numbers second. A quick visual pass settles the gross questions, the squeeze, the strain, the sac, the rough volume; only then does the clinician decide which one or two numbers the case truly needs. A breathless patient of doubtful volume earns a stroke distance and a leg raise; a patient with a strong pump and high pressure earns a filling ratio; few patients need every measure the machine can take.
Taking fewer numbers well beats taking many badly. Each measurement adds minutes and a fresh chance of error; the disciplined study takes the one or two that will change the plan and leaves the rest, the focused power of the handheld lying as much in what it skips as in what it measures.
Eyeball first; then the number the case needs.
Where the numbers mislead
Doppler is exquisitely sensitive to angle; that sensitivity is its commonest trap. The beam must run nearly parallel to the flow it measures, since a beam crossing the stream at an angle reads the speed too low, the error growing as the angle widens. A stroke distance taken off-axis underestimates the output and can fake a failing heart out of a sound one, the number wrong not because the heart is sick but because the beam was aimed askew. The remedy is patience with the alignment, fanning and steering until the trace runs sharp and tall, since the truest velocity is the highest a careful sweep can find; a low, blunt envelope is a sign the beam, not the heart, is at fault.
The single number in isolation is the other hazard. A filling-pressure ratio, an output, a stroke distance, each is one reading of a moving system and means little torn from the rest, weighed properly only against the eyeball picture, the chambers, the history and the trend across time. A number that disagrees with everything else on the screen is more often a measurement error than a discovery; the clinician who chases it past the plain picture has been fooled by the authority of a figure.
The reach and the limit of the measured exam
The advanced layer is where the focused scan stops guessing and starts measuring; at its best it answers questions the eyeball never could: how much blood the heart moves, how high the pressure behind it stands, whether the next litre of fluid helps or harms. A clinician who can take a clean stroke distance and a filling-pressure ratio at the bedside carries a small laboratory in one hand, the quantitative power that once lived only in the echo department brought to the trolley where the decision is made. The volume question answered by a leg raise, the stiff heart named by a filling ratio, the output trended through a resuscitation: each was once a trip down the corridor and is now a measurement taken where the patient lies.
The limit rides alongside the reach. The pocket machine does a fraction of what the cart does; the numbers it takes demand more care than the eyeball reads they refine. Used by a clinician who knows when a measurement earns its minutes, who aligns the beam and weighs the number against the whole, who hands the deeper quantification to the laboratory built for it, the handheld becomes more than a screening eye: it becomes a measuring one, as far as a pocket and a careful hand can take it. That is the honest boundary of the advanced bedside exam: real numbers in real time for the questions that change the plan, with a clear handoff to the laboratory for the depth a pocket was never built to reach. A clinician who carries that boundary in mind neither overreaches the pocket machine nor underuses it, taking the few numbers it takes well and sending the rest onward, the advanced bedside exam strongest when it knows its own edge. The measure that earns its minutes is the one to take; the rest can wait for the cart.