Infective Endocarditis Ultrasound Diagnosis Handheld Echocardiography
Infective endocarditis is an infection that has taken hold on a heart valve, building a clump of microbes and clot called a vegetation that chews the valve apart and flings showers of infected debris into the circulation. Echocardiography is the eye that watches the valve for that growth; in a feverish patient with a murmur it can be the look that turns a suspicion into a diagnosis. The handheld scan, on the chest, is a limited eye: it can catch a large vegetation and the wrecked valve behind it, but it can never, on its own, declare the valve clean. Knowing what the growth looks like, and knowing the hard limit of a surface scan that misses the small ones, is the whole of using ultrasound well in this disease.
The scan can find the infection; it cannot rule it out.
How each valve is brought cleanly into view, and how colour marks a leak across it, sits in the pages on the individual views. The work here is the growth itself, the damage it does, and the limit that governs every reading.
The vegetation and its impostors
The vegetation is the thing the scan hunts, and telling it from the harmless lumps that crowd an ageing valve is the skill the disease demands. A true vegetation has a set of habits the eye learns to read. It clings to a valve leaflet, usually on the upstream side, the face the blood strikes before the valve closes, the low-pressure side where the infection settles and grows. It is irregular and shaggy in shape, never the smooth line of a healthy leaflet, a ragged clump with no clean edge. Above all it moves, moving on its own: while the leaflet swings with the beat, the vegetation flutters and lashes independently, a mass with a motion of its own, oscillating in the blood like a flag in a gust. That independent, chaotic motion is the surest single mark, the one habit the impostors rarely manage. Size and number are read alongside shape: a vegetation a centimetre or more across, or several studding one valve, marks a heavier infection and a higher chance of pieces breaking free, where a small single growth is read with the same care but a lighter alarm. The valve carries a crowd of lookalikes that the unwary read as infection. A knob of calcium on an old valve sits bright and still, fixed to the leaflet, moving only as the leaflet moves, lacking the lashing freedom of a vegetation. A leaflet thickened by age or wear looks lumpy without being infected, its bulk part of the valve itself instead of a clump stuck upon it. Tiny filaments called Lambl’s excrescences trail from the closure line of normal valves, thin strands that a fearful eye magnifies into disease. A benign tumour of the valve, a fibroelastoma, can mimic a vegetation closely, mobile and attached, separated from it more by the company it keeps, the fever and the positive blood cultures, than by its look alone. And a vegetation already healed by treatment can sit on for months, dense and still, a scar rather than an active infection, indistinguishable on the screen from the growth it once was. Each of these is sorted less by a single feature than by the whole picture, the shape and the motion and the setting together, the lashing irregular mobile mass in a septic patient reading as infection where the bright fixed knob in a well one reads as old calcium.
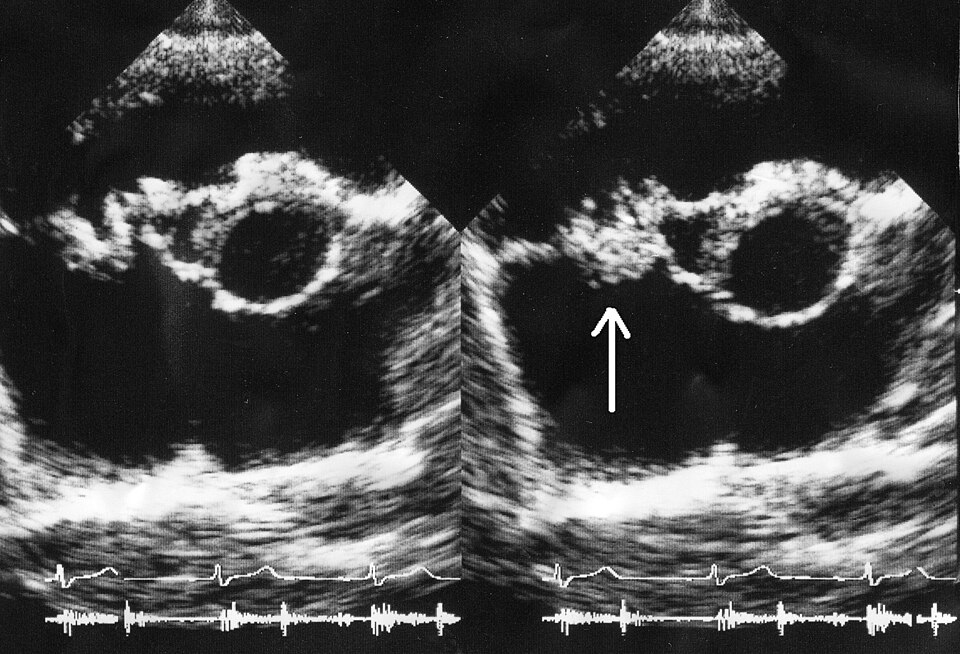
The vegetation lashes on its own; the impostors hold still.
The scan that cannot say no
The hardest truth of this disease is what a clean scan does not mean. A handheld surface scan catches the large, obvious vegetations and misses the small ones, the early ones, the ones tucked where the beam reads poorly, so a scan that shows nothing has not cleared the valve. In a patient whose fever and cultures point at endocarditis, a normal surface scan lowers the odds not at all; it simply means the growth, if there, is below what this tool can see. The numbers are sobering: a surface scan catches perhaps two in three native-valve vegetations and fewer of the small ones, a miss rate no clinician can treat as a clearance in a patient who fits the disease.
A negative bedside scan never excludes the disease.
The fuller answer comes from a probe passed down the gullet, behind the heart, close to the valves, a study far more sensitive to the small vegetation and the hidden abscess; the one that must follow when suspicion stays high or an artificial valve is in question. The surface scan, in the framework that diagnoses endocarditis, counts as one strong piece of evidence among several: a vegetation seen, an abscess, a new leak, a loosened artificial valve, each weighed alongside the blood cultures and the fever, the diagnosis built from the whole instead of from the image alone. A clinician who treats a bedside scan as the verdict, either way, has asked one limited tool to settle a question that needs the cultures, the story and often the deeper probe to answer. The timing matters as much as the tool: a first scan early in the illness can read clean and a repeat days later show a vegetation grown into view, so a suspicion that outlasts a negative scan earns a second look as the infection declares itself, the disease read over time and never frozen in one image.
What the infection wrecks
The growth is dangerous less for itself than for the ruin it works on the valve. The infection eats through the leaflet it sits on; a valve eaten through cannot seal: it springs a sudden, severe leak, blood pouring backward through a valve that no longer closes, a flood the heart was never built to take all at once. That acute leak, more than the vegetation, is what tips an endocarditis patient into breathlessness and shock, the bedside finding that turns a stable infection into an emergency. The speed is the danger: a chronic leak the heart has had years to adapt to is borne, where the same volume arriving overnight floods a stiff, unprepared chamber and backs straight into the lungs. A new, severe, sudden leak in a febrile patient is a surgical emergency in the making.
Colour laid over the wrecked valve shows the leak at once, a wide spray where the seal has failed, the reading detail belonging to the view pages.
The destruction takes other forms the scan should seek. A leaflet can tear through and perforate, a hole opening mid-leaflet where the infection burrowed. A leaflet’s supporting cords can snap, leaving it flailing loose into the chamber behind. Worst of all, the infection can burrow off the valve into the surrounding tissue and hollow out an abscess, a pocket of pus beside the valve ring that carries a grim outlook and often a need for surgery, sometimes pressing on the heart’s wiring until the beat itself falters. A scan that finds a wrecked valve or a pocket beside it has found a patient who needs the surgeons, not just the antibiotics. The abscess earns the closest look, since it hides off the valve in tissue the surface scan reads poorly; a fever that will not settle on good antibiotics is itself a hint to hunt for the pocket the bedside may have missed.
The debris that travels
A vegetation is a loose clump in a fast current; pieces break off and sail away. A fragment thrown from a valve on the left side of the heart rides the arteries to the brain, the spleen, the kidney, lodging as a stroke or an infarct far from the heart that launched it, the embolic risk climbing with the size and the wildness of the growth. A large, mobile vegetation is watched with special unease, since the bigger and freer it is the more likely a piece tears loose; an embolus to the brain can be the first sign of an endocarditis still unsuspected, the stroke arriving before the fever is explained.
The right side of the heart tells a different version of the same story. An infection on the tricuspid valve, common in a patient who injects drugs into their veins, throws its debris not to the brain but to the lungs, seeding showers of septic clots that stud the lung with infarcts and abscesses. A breathless, feverish patient who injects drugs, with patches scattered through the lungs, is a patient whose tricuspid valve the scan should study with care. The lungs in that patient carry the evidence the heart launched, round shadows and wedge-shaped infarcts scattered through both fields, a lung picture that should send the eye straight back to the right-sided valves for the source.
Bits break off and lodge wherever the blood carries them.
Where it misleads
The lookalikes catch the eager. A clinician hunting endocarditis can read a knob of calcium, a thickened leaflet, a wisp of normal tissue as the growth they fear, then start a long course of treatment for an infection that is not there. The guard is the whole picture: the lashing motion, the irregular shape, the upstream attachment, read together and against the fever and the cultures rather than off the screen alone. A lump unchanged on every old scan in the file is old; a lump new since the last study, in a patient now febrile, is the one to fear, the comparison with any earlier image telling more than any single feature.
The graver error runs the other way. A clinician who scans a septic patient, sees a clean valve, then crosses endocarditis off the list has trusted a tool past its reach, since the surface scan misses exactly the small early growth a high suspicion is hunting for. A negative scan in a patient who fits the disease is a reason to reach for the deeper probe, never a reason to stop. The artificial valve compounds the trap, its bright material scattering the beam and hiding the growths the scan is asked to find. An artificial valve in a febrile patient is a near-automatic reason to send for the deeper probe, the surface scan all but blind to the growth and the loosening that ring can hide.
The eye on the valve and its blind spot
The bedside scan earns its place in endocarditis by catching the findings that change the night. A large vegetation lashing on a valve, a leaflet wrecked into a sudden flood of backward flow, a pocket of pus beside the valve ring: any of these, seen on a handheld scan in a septic patient, turns a slow workup into an urgent call to the cardiologists and the surgeons, the probe buying hours that matter in a disease that destroys valves fast.
The blind spot is the other half of the lesson. The surface scan sees the loud findings and misses the quiet ones, names the disease when it catches the growth and stays silent, never safe, when it does not. Used as one piece of evidence among the cultures and the fever and the deeper study, read for what it can show and distrusted where it cannot, the handheld scan is a fast and powerful eye on a sick valve, as long as the clinician remembers it is an eye that can be fooled and an eye that can be blind. The clinician who carries both halves of that lesson, trusting a loud finding and doubting a quiet one, gets the best from a tool that can save a valve and a life when it sees and that hands the patient onward, never dismisses them, when it does not. In a disease that wrecks valves in days, that balance of nerve and humility is the reading that counts, a scan that serves the patient far better than one read with confidence alone.