Atrial Fibrillation Handheld Echocardiography Assessment Protocol
Atrial fibrillation is named by the tracing, not the probe. The diagnosis lives on the electrocardiogram, in the irregular, disorganised line that marks an atrium quivering instead of beating. What the probe adds is everything the tracing cannot say: why the atrium fell into fibrillation, what the rhythm has done to the heart over the months it has run, and what danger it now poses. A handheld scan in a patient with atrial fibrillation is a hunt for the cause behind the rhythm, the damage beneath it, and the clot it may be brewing, bounded by a hard limit on the one thing it cannot see.
The tracing names the rhythm; the probe reads its meaning.
How each chamber, wall and valve is measured sits in the pages on the individual views. The work here is the questions atrial fibrillation raises and how the scan answers them, including the one it cannot.
The rhythm the probe does not name
The scan does not diagnose the fibrillation. By the time the probe is on the chest the rhythm is already known from the monitor, the irregular pulse felt at the wrist, the chaotic tracing on the screen. Asking ultrasound to confirm a rhythm is asking the wrong tool the wrong question. The probe reads structure and flow, never the electrical storm in the atrial wall; the irregular pulse and the chaotic line have already settled what kind of rhythm this is before the gel touches the skin.
What the scan answers is what the rhythm leaves unanswered. Is the atrium fibrillating because a valve is failing or a ventricle is stiff. Has the fast, disorganised beat begun to weaken the pump. Is a clot forming in the still corners of an atrium that no longer empties cleanly. Those are the questions the probe is brought to settle; each has a place in a fixed round of looking. The round is short: the atrium for its size, the valves for a cause, the ventricle for its strength across several beats, the deep corners for the haze of stalled blood.
Rhythm to the tracing; cause and consequence to the probe.
Reading a heart that will not keep time
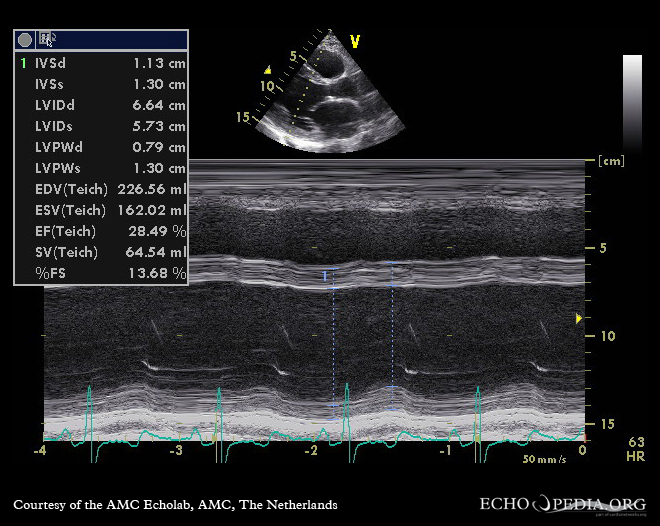
The first thing the fibrillating heart does to the scan is break the steady rhythm every measurement quietly assumes, and reading around that irregularity is the skill the rhythm demands. A normal heart beats evenly, each filling the same as the last, so a single beat read off the screen stands for all of them. Atrial fibrillation destroys that evenness: the beats come at random intervals; the strength of each depends on how long the heart had to fill before it. A beat that follows a long pause has had time to fill generously and squeezes hard, ejecting a large volume and flashing a strong, brisk picture on the screen; a beat that follows a short interval has barely filled and squeezes weakly, a feeble picture a moment later. Read a single beat in atrial fibrillation and the reading is a lie, since the next beat may tell the opposite story; the long-pause beat flatters a failing ventricle into looking vigorous, the short-interval beat slanders a strong one into looking weak. The fix is to stop trusting any one beat. A clinician judging the pump in atrial fibrillation watches across many beats, five or more, taking the average impression over the best or the worst, letting the eye settle on the typical squeeze instead of the extremes. A more careful reading picks an index beat, one whose two preceding intervals are roughly equal and average, reading function from that, the beat that best represents a heart filling neither too long nor too little. The same caution governs every Doppler measure of flow, each of which swings with the interval before it and must be averaged the same way. The strong beat after a pause carries its own trap, a potentiated squeeze that can make a weak heart look fixed when rate control might yet recover it, so the post-pause beat is read with suspicion rather than relief. A clinician who forgets the irregularity reports a heart that does not exist, vigorous or failing by the accident of which beat the eye happened to land on, when the truth lay in the average the irregular rhythm hid.
No single beat tells the truth in fibrillation.
Why the atrium fibrillates
The scan’s first hunt is for the cause, since atrial fibrillation rarely arrives without a reason written in the heart. A left atrium stretched wide is the commonest footprint, an atrium enlarged over years by a pressure or a leak behind it, the chamber that both suffers and drives the fibrillation. A thickened ventricle, stiffened by long-standing high pressure, fills poorly and backs that pressure up into the atrium until it gives way to the rhythm. A muscle thickened or scarred, a pericardium gripping the heart, a long-standing leak of any of the valves: each loads the atrium over time until its wall, stretched and remodelled, loses the orderly beat and falls to fibrillation. The scan reads these slow causes in the size and the walls the rhythm has shaped.
The valves carry their own share of the blame. A mitral valve narrowed by old rheumatic disease dams blood behind it and swells the atrium until it fibrillates, a cause the focused scan should always seek in a younger patient with a new irregular rhythm. How that valve and that atrium are measured belongs to the view pages; the embolism the scan looks for here is the cause, read off chambers the rhythm has marked.
A wide atrium is the rhythm’s signature.
The cause matters because it steers the treatment. A fibrillation driven by a fixable valve points one way, a fibrillation riding on a stiff hypertensive heart another, and a structurally clean heart in new fibrillation a third. The scan that names the cause shapes the plan that follows, the rhythm read not as an isolated electrical fault but as the surface mark of something structural underneath. A first scan in new fibrillation is also a baseline, the atrium and the ventricle measured now so a later scan can show whether they have stretched further or held, the rhythm tracked by its slow footprint on the chambers.
The clot the probe cannot see
The gravest danger of atrial fibrillation is the clot; here the handheld scan meets its hardest limit. When the atrium quivers instead of contracting, blood stalls in its still corners; in the worst corner of all, a small pouch off the left atrium called the appendage, that stalled blood can clot into the source of a stroke. The appendage is where the clot forms first of all, the one corner a probe on the chest cannot reach: it sits tucked behind the heart, screened from a surface scan, visible only to a probe passed down the gullet behind it.
The handheld scan cannot clear the atrium of clot.
This limit has a sharp clinical edge. Before the rhythm is shocked back to normal in a patient who has been fibrillating for more than a day or two, the appendage must be known to be free of clot, since the returning contraction can fling a waiting thrombus into the circulation as a stroke. That clearance comes from the probe down the gullet or from weeks of blood-thinning, never from the handheld scan on the chest. A clinician who reads a clean surface scan as permission to shock a long-standing fibrillation has misunderstood the tool, mistaking the corner it cannot see for a corner that is empty.
Sometimes the surface scan hints at the danger without naming the clot. Blood stalling in a dilated atrium can swirl into a faint, smoke-like haze on the screen, a sign of the sluggish flow that breeds thrombus, a warning the appendage may be loading even when the surface probe cannot look inside it.
The lost beat costs more than a clot in some hearts. A stiff, thick or stenosed heart leans hard on the atrium’s kick to fill its ventricle; when fibrillation steals that kick the output can fall sharply, the patient tipping from coping to crashing as the rhythm takes hold. A scan that shows a small, stiff ventricle behind a new fibrillation explains a collapse the rate alone would not.
Rate, rhythm, the weakened pump
A fast fibrillation left to run can wear the pump down. A ventricle driven too quickly for too long tires and dilates, its squeeze fading into a weakness that looks for all the world like a failing heart muscle, when the cause is simply a rate never brought under control. The scan shows the weak, dilated ventricle; the rhythm strip shows the relentless rate driving it.
The hopeful part is that this weakness can lift. A pump worn down by an uncontrolled rate often recovers much of its strength once the rate is slowed or the rhythm restored, a reversible weakening instead of a fixed disease. The scan that finds a weak ventricle in a fast fibrillation flags a heart to recheck after the rate is controlled, the recovery on the follow-up scan confirming the cause. The catch is telling this reversible weakness from a fixed one at the first look, since the two wear the same face; the rate, the history and the recheck after control sort the heart that will mend from the heart that will not.
The reading guides the choice between slowing the rate and restoring the rhythm. A structurally sound heart with a recent fibrillation may tolerate an attempt to return it to a normal rhythm; a dilated atrium and a worn ventricle, long in fibrillation, lean toward controlling the rate and thinning the blood instead. The scan lays out the structure on which that choice rests.
Where it misleads
The irregular rhythm is the great deceiver. A single beat read in haste, a strong one after a pause or a weak one after a short interval, reports a pump that is not there; a clinician who measures one beat and moves on carries away a number the next beat would have overturned. The average across beats is the only honest reading; the discipline of taking it is the heart of scanning a fibrillating patient.
The clot is the other trap, the more dangerous of the two. A clean surface scan says nothing about the appendage it cannot see; reading it as a clearance to shock a long-standing rhythm risks the stroke the caution was built to prevent. The handheld scan names the cause and the consequence of atrial fibrillation; it does not and cannot vouch for the corner where the clot hides.
What the scan settles, what it leaves
The bedside scan turns atrial fibrillation from a line on a tracing into a heart understood. It names the cause behind the rhythm, the stretched atrium and the failing valve and the stiff ventricle; it weighs the consequence, the pump worn thin by an uncontrolled rate; it warns of the stasis that breeds a clot. In minutes at the bedside it gives a clinician the structural picture on which the whole plan of rate, rhythm and blood-thinning is built.
The limit is as important as the reach. The scan reads the cause and the damage of the fibrillation, reading them best when the clinician remembers to average the irregular beats rather than trust one; it cannot see into the appendage where the clot waits; it never pretends to. A tool that knows what it cannot do is the one that keeps the patient safest, the surface scan handing the question of the hidden clot to the probe and the time that can answer it. Read for what it can give and trusted no further, the bedside scan in atrial fibrillation is among the quickest ways to turn a rhythm into a plan. It reads the heart the rhythm has shaped and stops honestly at the one door it cannot open.